Sixty-One Statements, Three Certainties: What the Surviving Sepsis Campaign 2026 Pediatric Sepsis Guidelines Say About the Evidence We Do Not Have
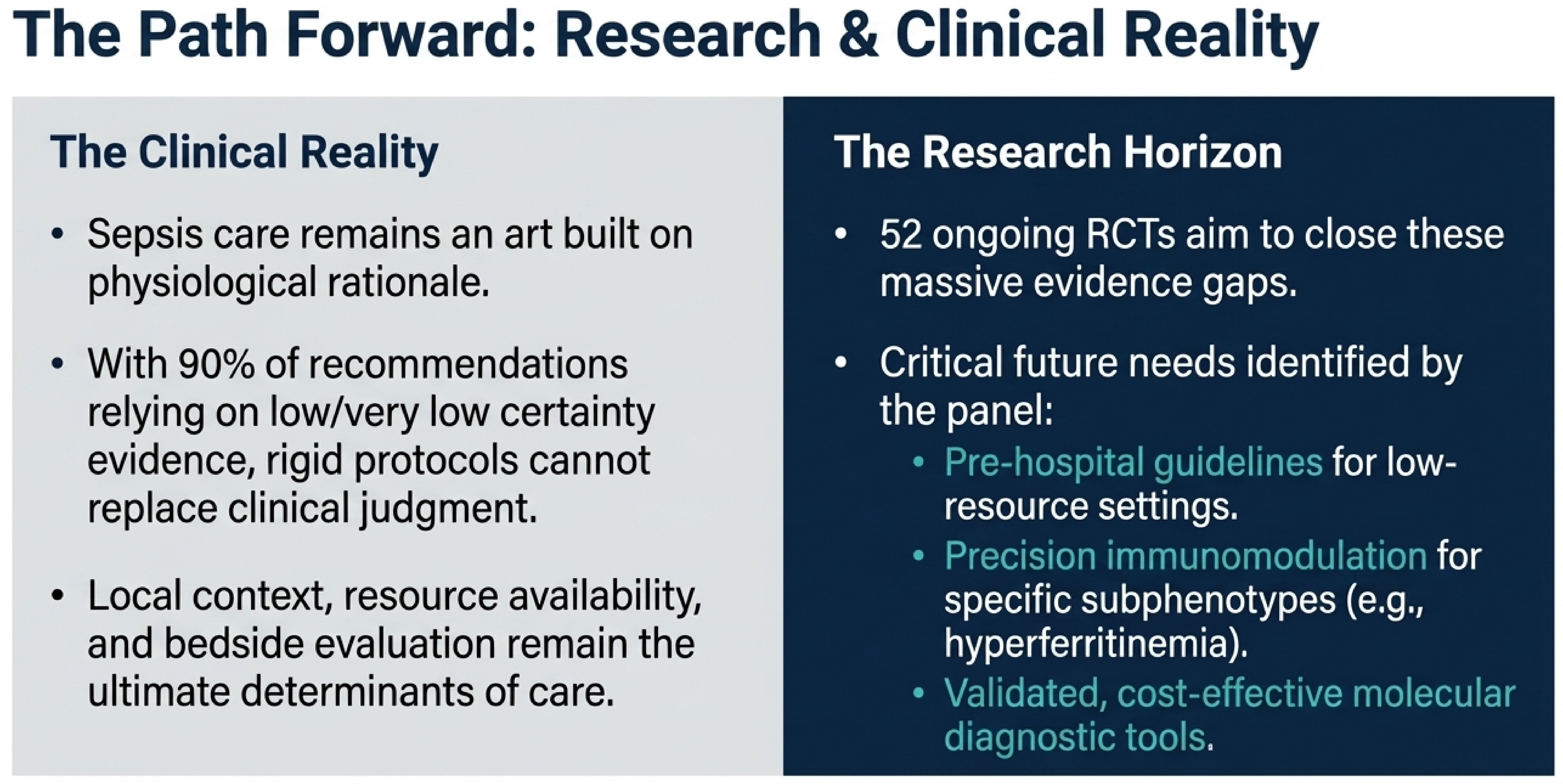
When the world's most authoritative guideline on pediatric sepsis acknowledges that 90% of its recommendations rest on low or very low evidence,it is issuing an invitation..!

The principal contribution of this guidelines lies in its legitimacy and scope. It is neither a local consensus statement nor the opinion of a single professional society. Rather, it represents a synthesis of input from 68 international experts representing 13 professional organizations, covering pediatric critical care, emergency medicine, infectious diseases, nursing, and psychology. The initiative was funded entirely by the European Society of Intensive Care Medicine (ESICM) and the Society of Critical Care Medicine (SCCM), with no industry support. This funding structure removes a potential source of commercial bias. Accordingly, this independence is relevant for those applying the recommendations in clinical practice or educational settings.
SSC 2026 Pediatric Guidelines — At a Glance
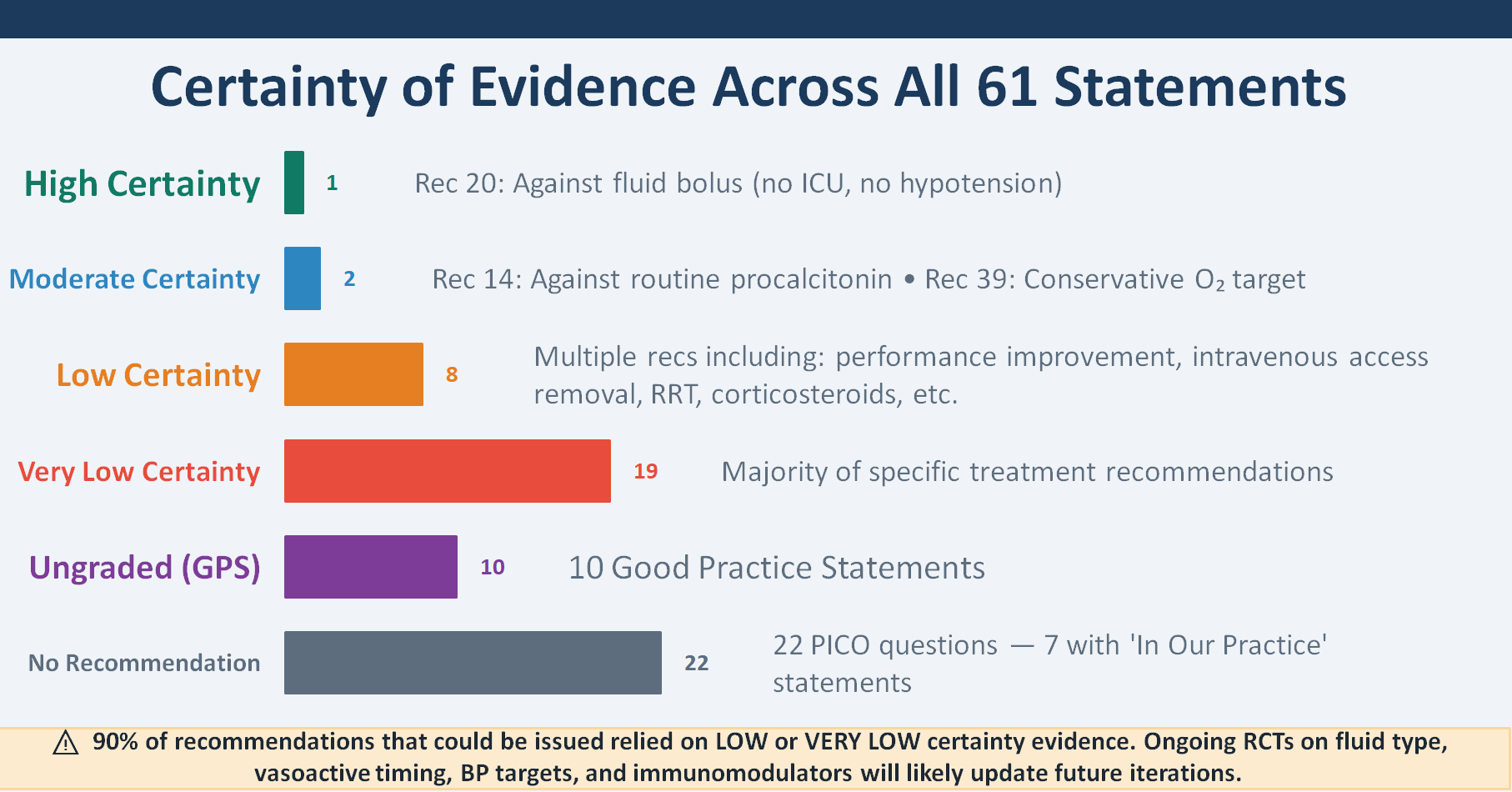
The primary teaching/learning point is that only 3 of 61 statements are based on high or moderate certainty evidence. The remaining statements rely on low, very low, or absent evidence. This reflects the current state of the field rather than a flaw in the guideline. The 2026 guidelines also demonstrate intellectual evolution: 20 recommendations are new, and 13 have been updated. The 22 statements carried forward without review indicate areas where no new evidence has emerged.

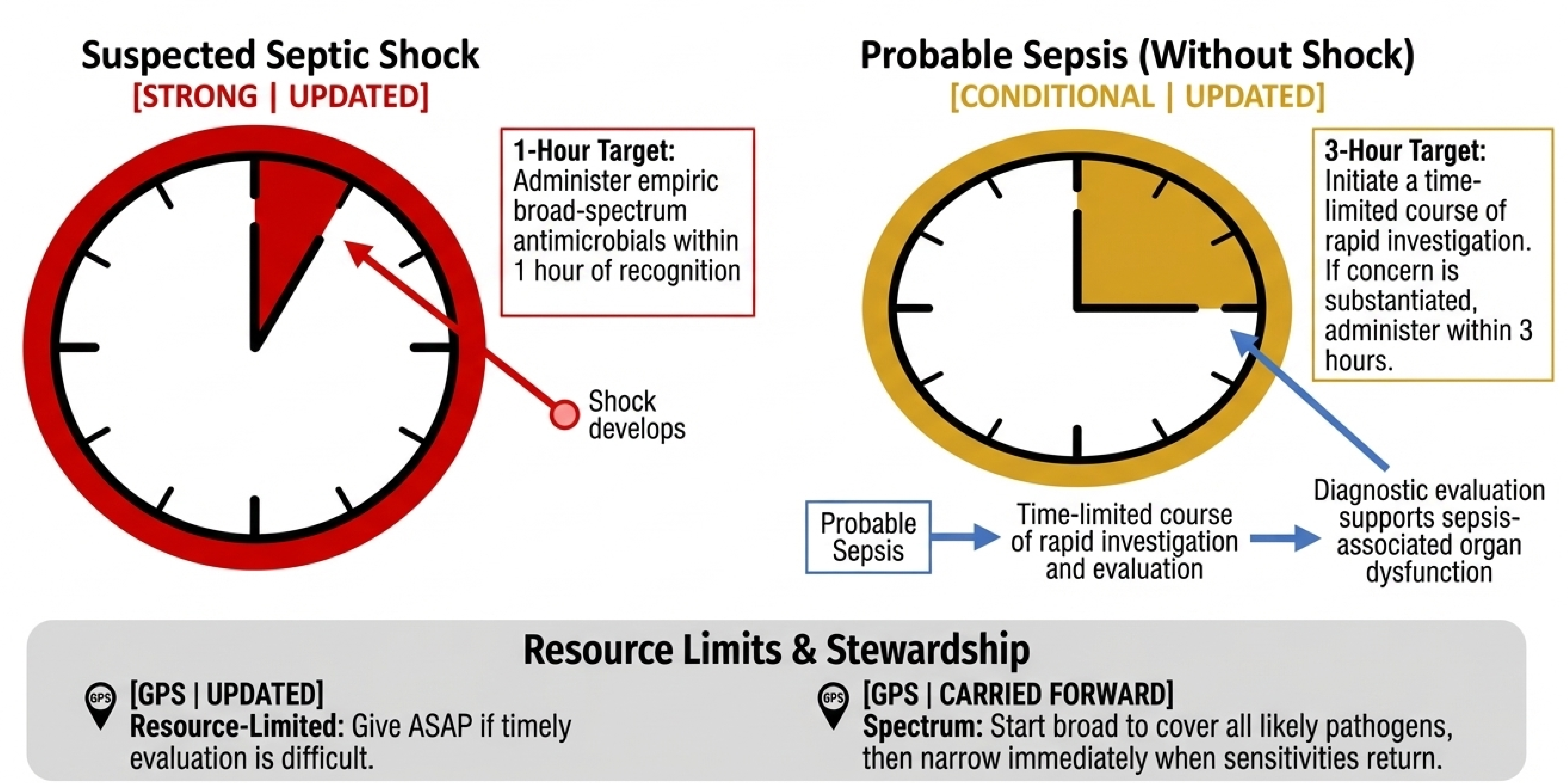
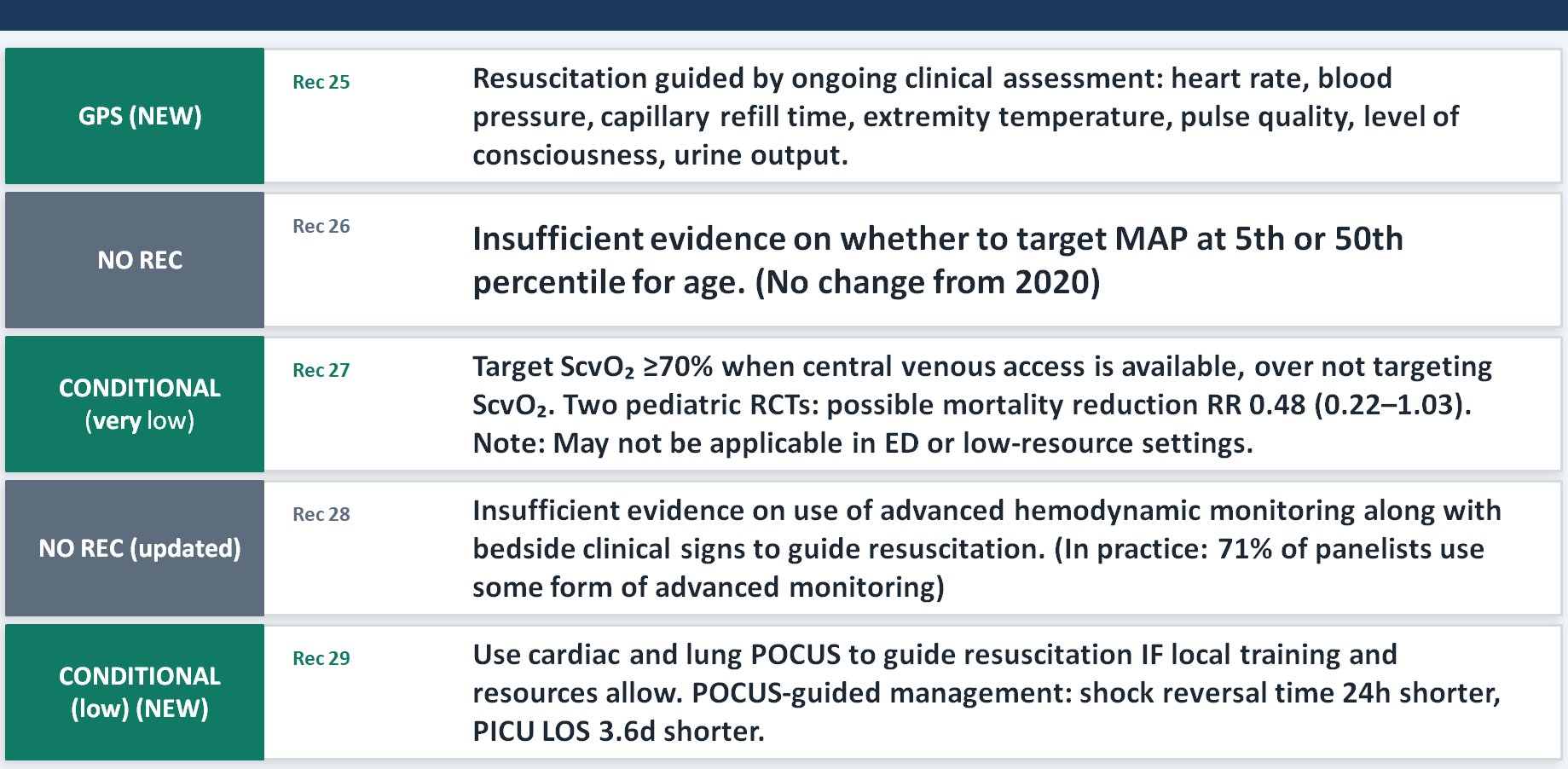
Quick guide for initial resuscitation in children with probable sepsis without shock or suspected septic shock.
A summary of key recommendations for recognition and resuscitation with indications of the strength of recommendations. Fluid bolus therapy and vasoactive administration should be continuously reassessed.

Evidence Quality — What the Data Tell Us
This should be shown to anybody who interprets a guideline recommendation as equivalent to proven efficacy. While summary statistics suggest low certainty, the visual presentation clarifies the extent: 19 of 61 statements are based on very low certainty evidence, and 22 PICOs yielded no recommendation at all. Epistemologically, this indicates that much of pediatric sepsis management derives from biological plausibility, adult data, and expert consensus rather than rigorous pediatric randomized trials. The panel explicitly identifies ongoing and needed trials—including PRoMPT BOLUS, SQUEEZE, and immunostimulant trials—as a research agenda.
Sepsis Definitions & Terminology (2024 Phoenix Criteria)
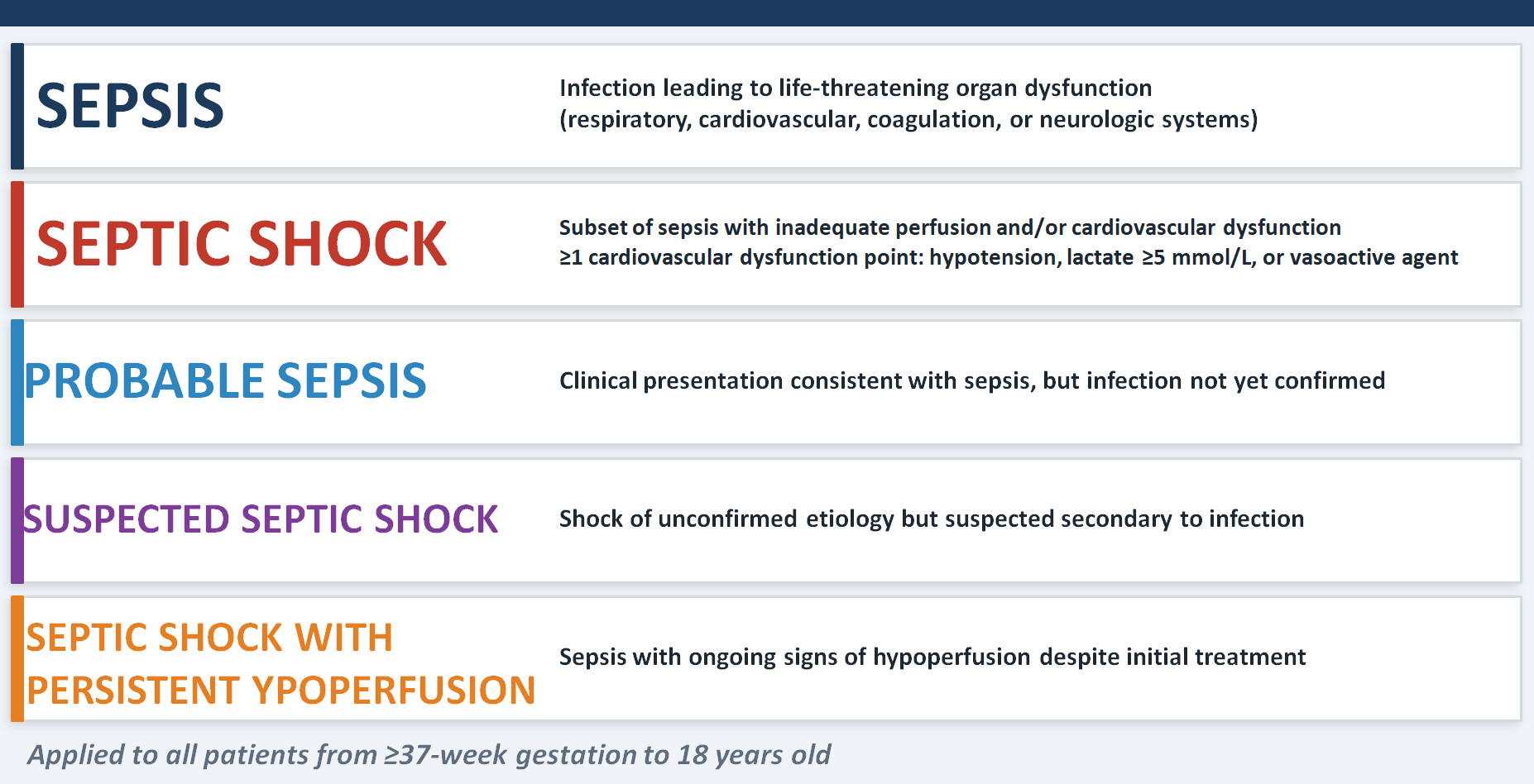
The key pedagogical message is the shift from 2005 IPSCC criteria to the 2024 Phoenix criteria, which operationalizes sepsis as organ dysfunction across four systems — respiratory, cardiovascular, coagulation, and neurological — rather than anchoring it to the older SIRS-based framework.
The most clinically practical point is how septic shock is now operationalized: at least one cardiovascular dysfunction point, meaning hypotension, lactate ≥5 mmol/L, or need for a vasoactive agent — any one of these three qualifies. Notice also the nuanced language the panel introduced: "probable sepsis" and "suspected septic shock." These terms matter because children present before confirmation is possible, and the guidelines are designed to be actionable in that uncertainty.
Recognition & Management of Infection
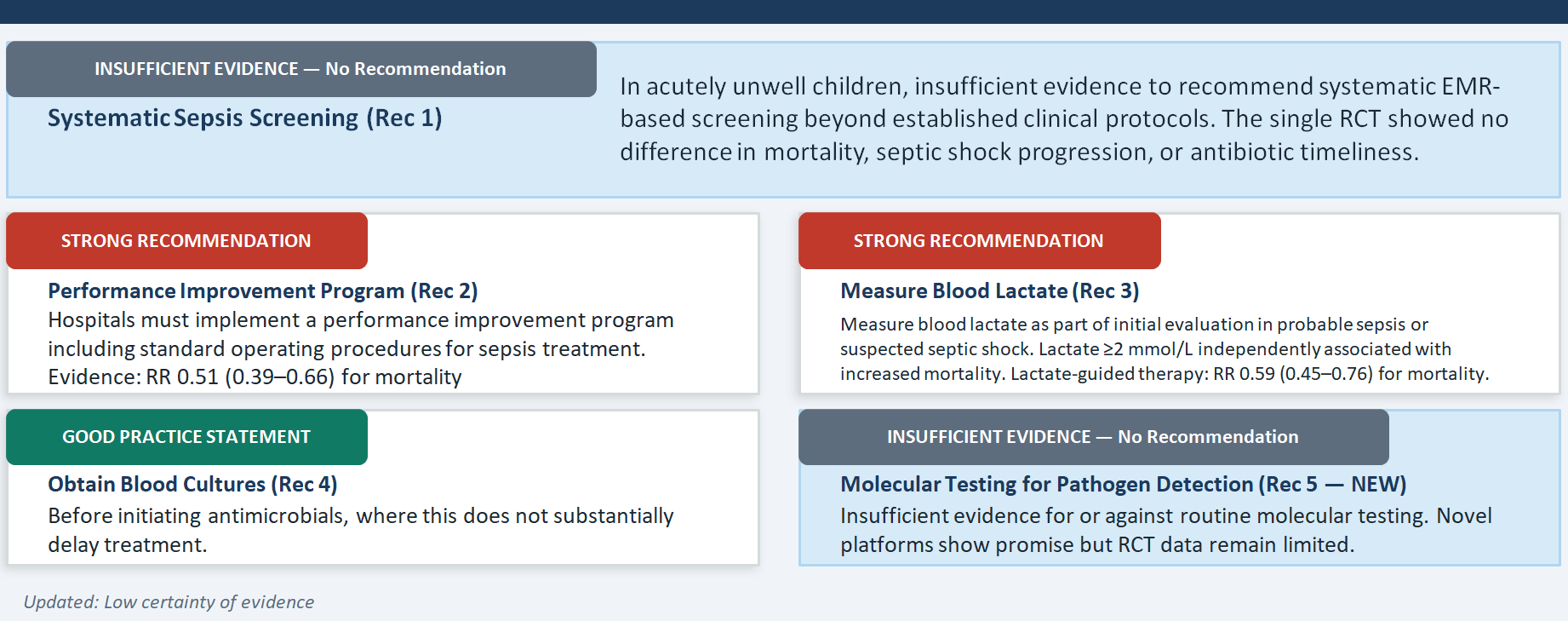
There are two important messages here that pull in slightly different directions. The first is the retreat from the 2020 guideline's suggestion to implement systematic sepsis screening — a rare case of a guideline being downgraded rather than upgraded. The only pediatric RCT with randomized allocation to EMR-based screening versus no screening found no difference in mortality, septic shock progression, or antibiotic timeliness. This should prompt honest institutional reflection about whether alert-heavy screening systems are delivering value. The second message, which the panel emphasizes strongly, is that this retreat from systematic screening does not mean passive waiting — it means building robust clinical protocols for recognizing acutely unwell children, and it means measuring blood lactate in all children with probable sepsis, which received a strong recommendation despite only very low certainty evidence. The biological rationale — lactate as a marker of tissue hypoperfusion and as a Phoenix criterion for cardiovascular dysfunction — is compelling enough to act even without RCT-level proof.
Antimicrobial Therapy — Timing & Initiation
For septic shock: 1 hour, strongly, no equivocation. For probable sepsis without shock: 3 hours, but the panel deliberately inserts a "time-limited course of rapid investigation" — meaning you should be asking whether this is actually sepsis, whether this might be viral, whether an antibiotic is truly necessary. This nuance is clinically important and often lost in the rush to comply with time metrics. The panel even notes — explicitly — that both very early antibiotic administration (under 30 minutes) and very late administration (over 330 minutes) were linked to mortality compared with intermediate timing, which tells us that panic-driven, reflex prescribing is also harmful. The GPS for resource-limited settings acknowledges the real world: when diagnostic testing simply isn't feasible, give antibiotics as soon as possible.
Antimicrobial Therapy — Empiric Coverage & De-escalation
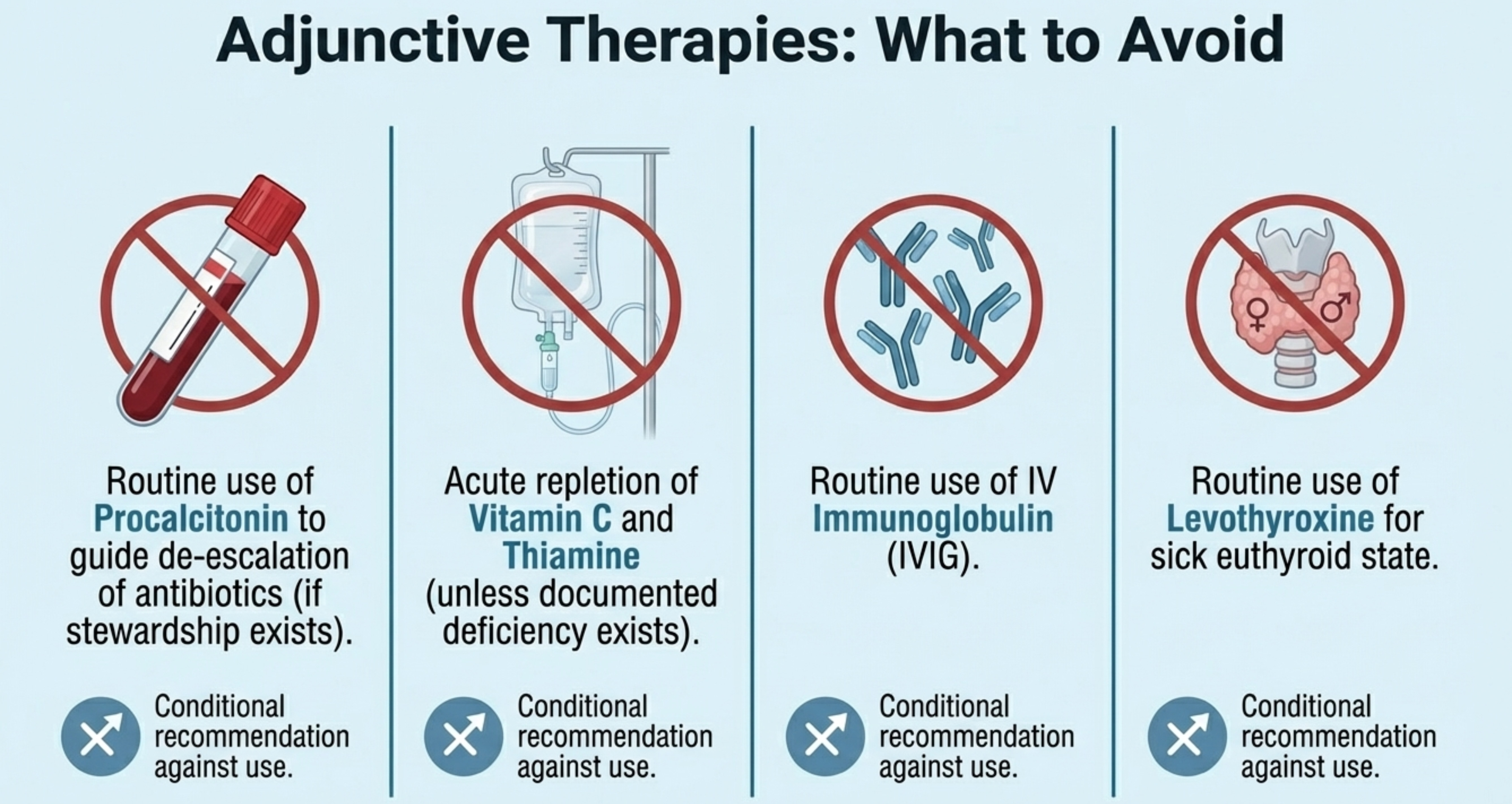
A new recommendation on procalcitonin (Rec 14), which is a conditional recommendation against its routine use for de-escalation when effective stewardship programs are already in place. This is counterintuitive to many, because procalcitonin has been widely promoted. But the pediatric RCTs showed no benefit in mortality or antibiotic duration when compared with mature antimicrobial stewardship infrastructure — and this is the key qualifier. Procalcitonin may add value where stewardship is weak, but where it is strong, the biomarker adds cost without benefit. The second important message is the new conditional recommendation for routine infectious diseases consultation when bloodstream infection is documented (Rec 15), with a pooled mortality benefit of RR 0.51. This is strong enough to be a service delivery argument: ID consultation should be the institutional standard for bacteremia, not an optional referral.
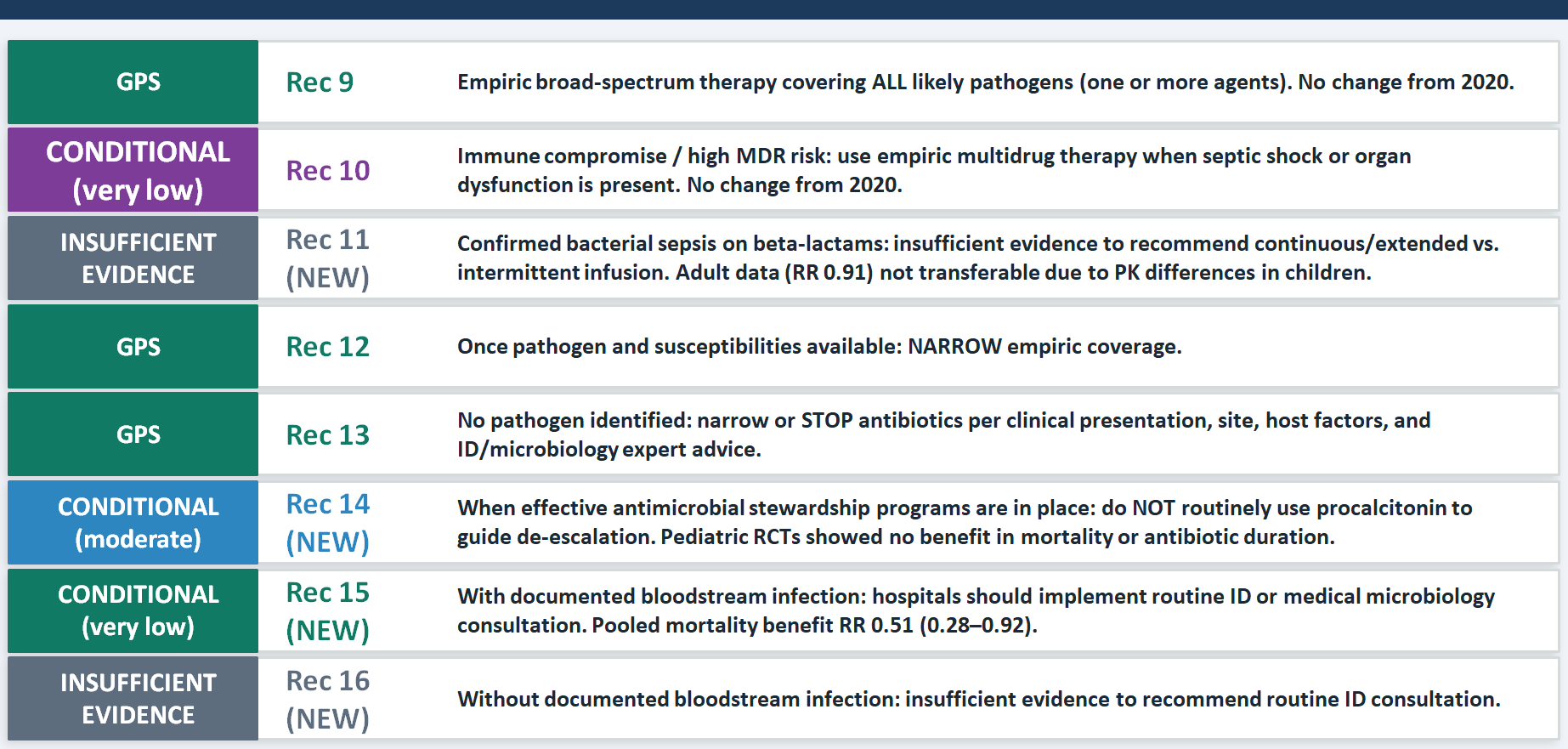
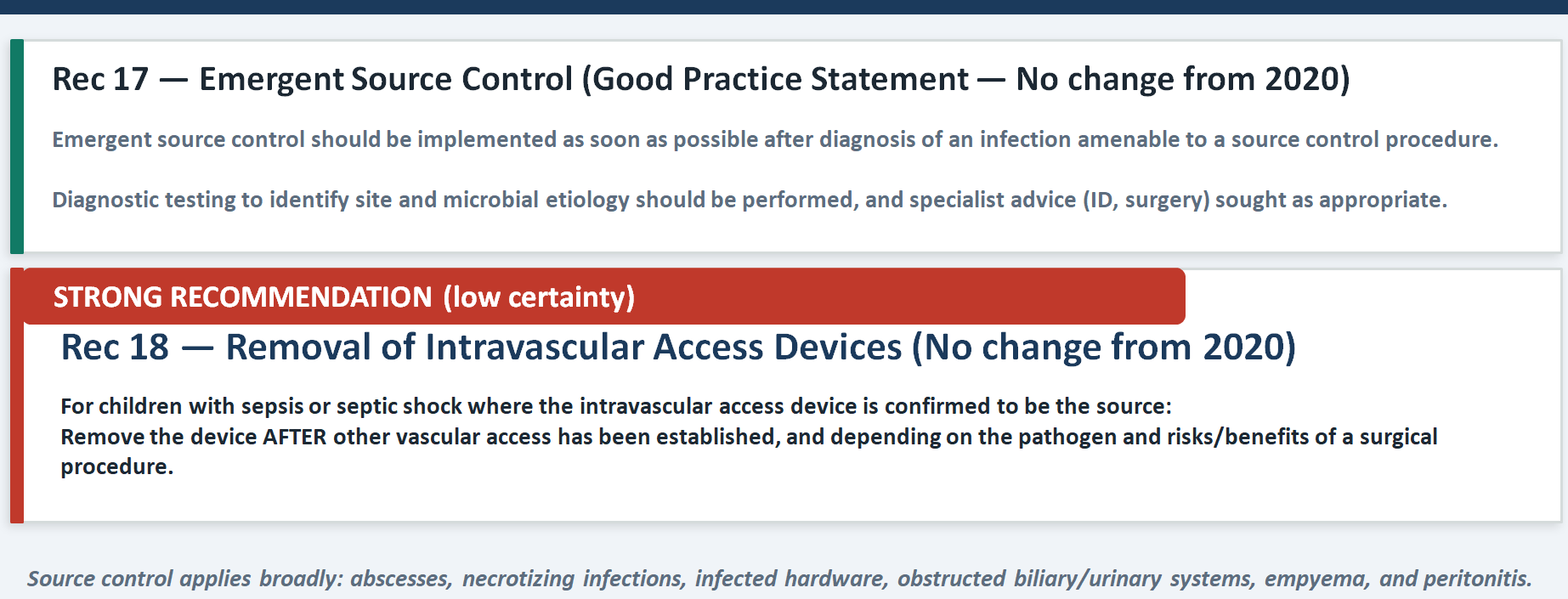
Source Control
No amount of fluid and antibiotics will rescue a child whose source has not been controlled. The strong recommendation to remove infected intravascular access devices (Rec 18) carries low certainty of evidence but was issued as a strong recommendation because the logic is biologically unassailable — you cannot cure catheter-related bacteremia while leaving the catheter in place. The practical teaching point is that source control decisions require multidisciplinary judgment: the treating clinician must engage surgery and infectious diseases early, and the risks of the procedure must be weighed against the risks of leaving the source untreated.
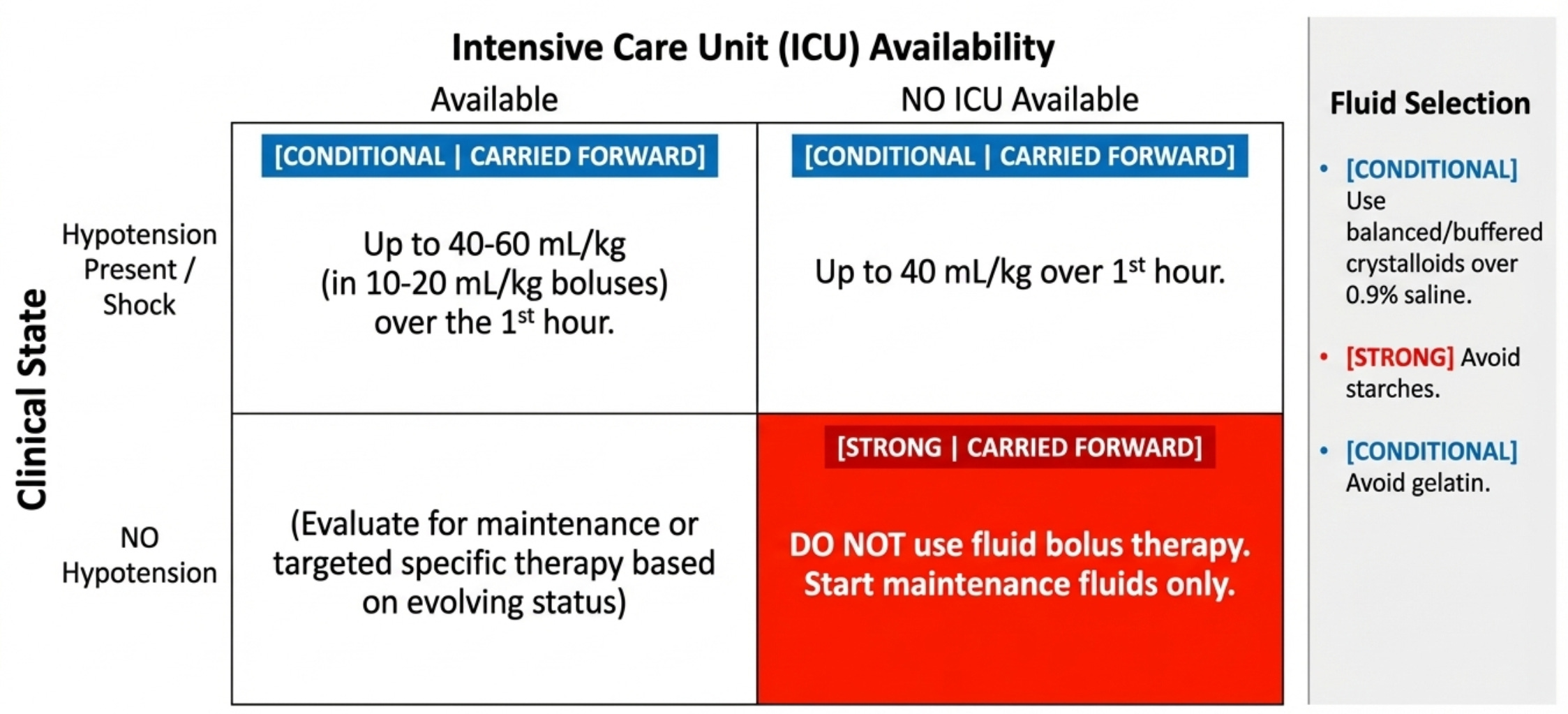
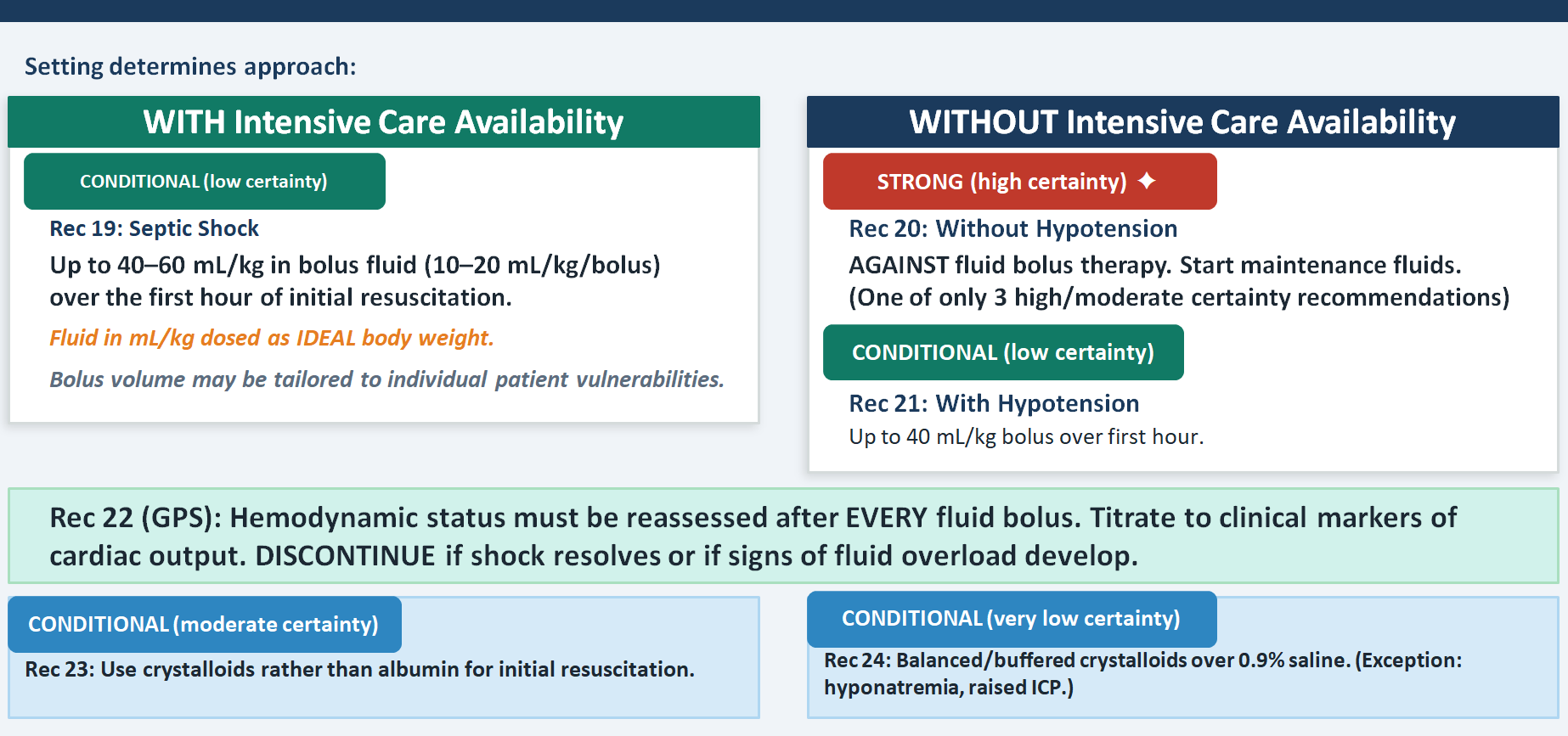
Fluid Therapy — Resuscitation Recommendations
This is one of the most practically transformative recommendations . The strong recommendation against fluid boluses in the absence of hypotension in settings without intensive care availability (Rec 20) is one of only three recommendations in the entire guideline that rests on high certainty evidence — drawn from the FEAST trial and its legacy. This directly overturns decades of PALS teaching that "fill the tank first." In high-resource settings with ICU backup, the conditional recommendation for up to 40–60 mL/kg over the first hour remains, but it is accompanied by two important nuances: dose on ideal body weight, and individualize to patient vulnerabilities. The crystalloid versus albumin recommendation (moderate certainty) and the balanced versus saline recommendation are both conditional — meaning the answer changes with context: a child with hyponatremia or raised intracranial pressure may actually need 0.9% saline.
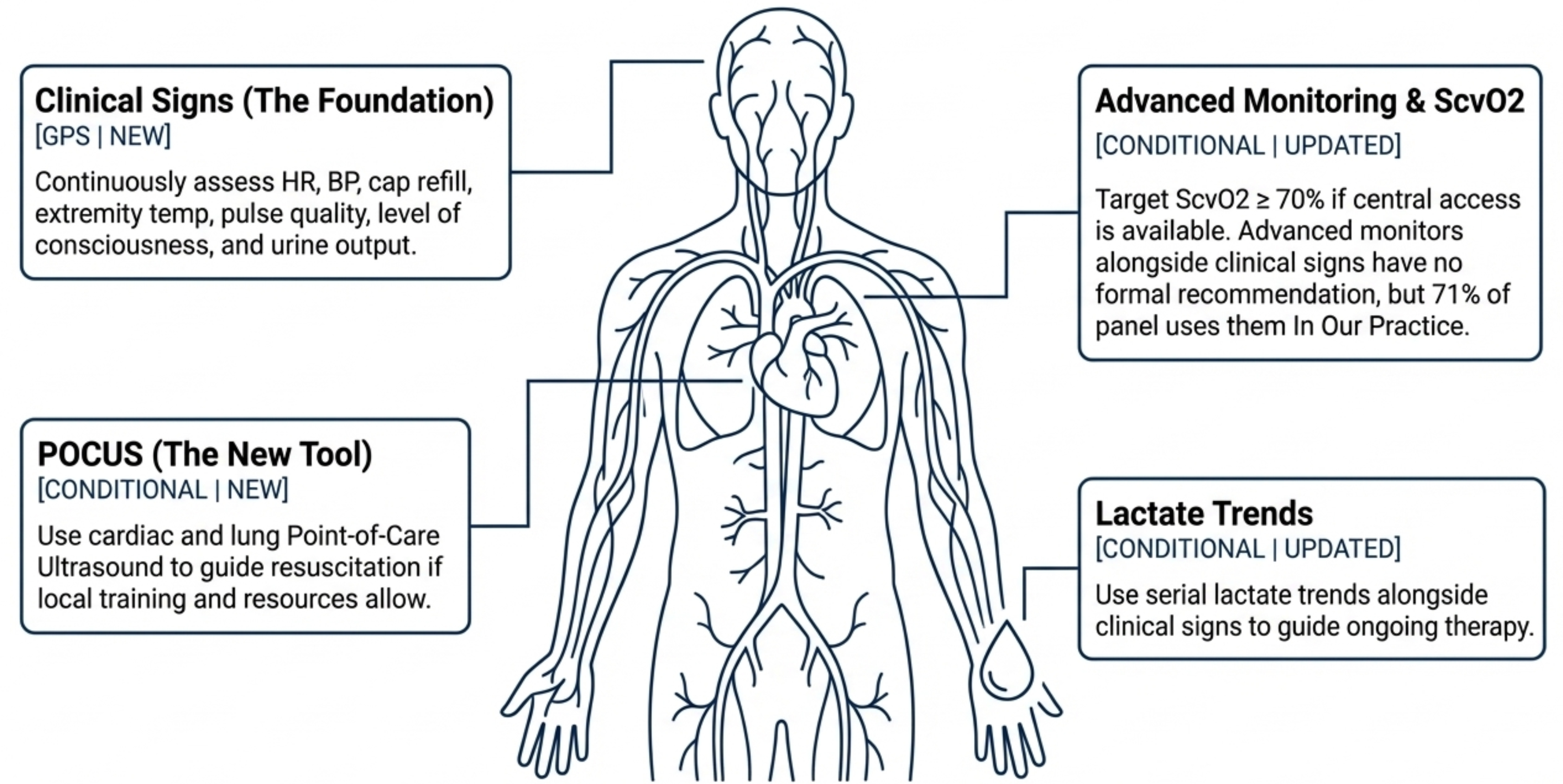
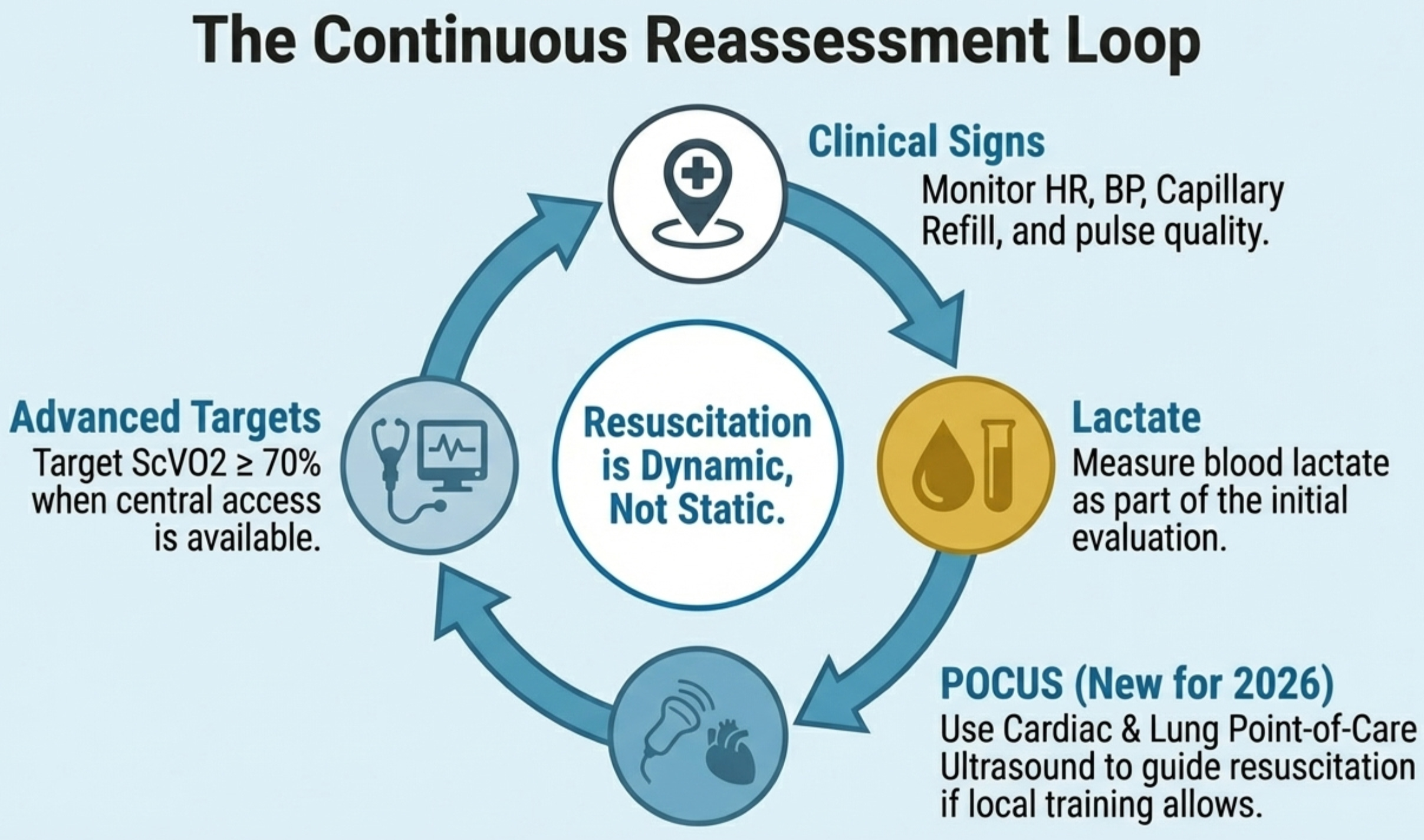
Hemodynamic Monitoring
The key update is the hierarchy of monitoring: start with clinical assessment (Rec 25, GPS), use ScvO₂ ≥70% as a target when you have central access (conditional, very low certainty), reach for POCUS when training allows (conditional, low certainty, and genuinely useful — changes clinical assessment in two-thirds of cases), and recognize that advanced hemodynamic monitoring beyond this has insufficient evidence to mandate (Rec 28). The pedagogical point is that expensive technology does not automatically improve outcomes if it is not embedded in a well-trained clinical framework. The retreat from earlier EGDT-style "target everything" protocols is reflected here — even ScvO₂, which was once considered the cornerstone of goal-directed therapy, now carries only a conditional recommendation.
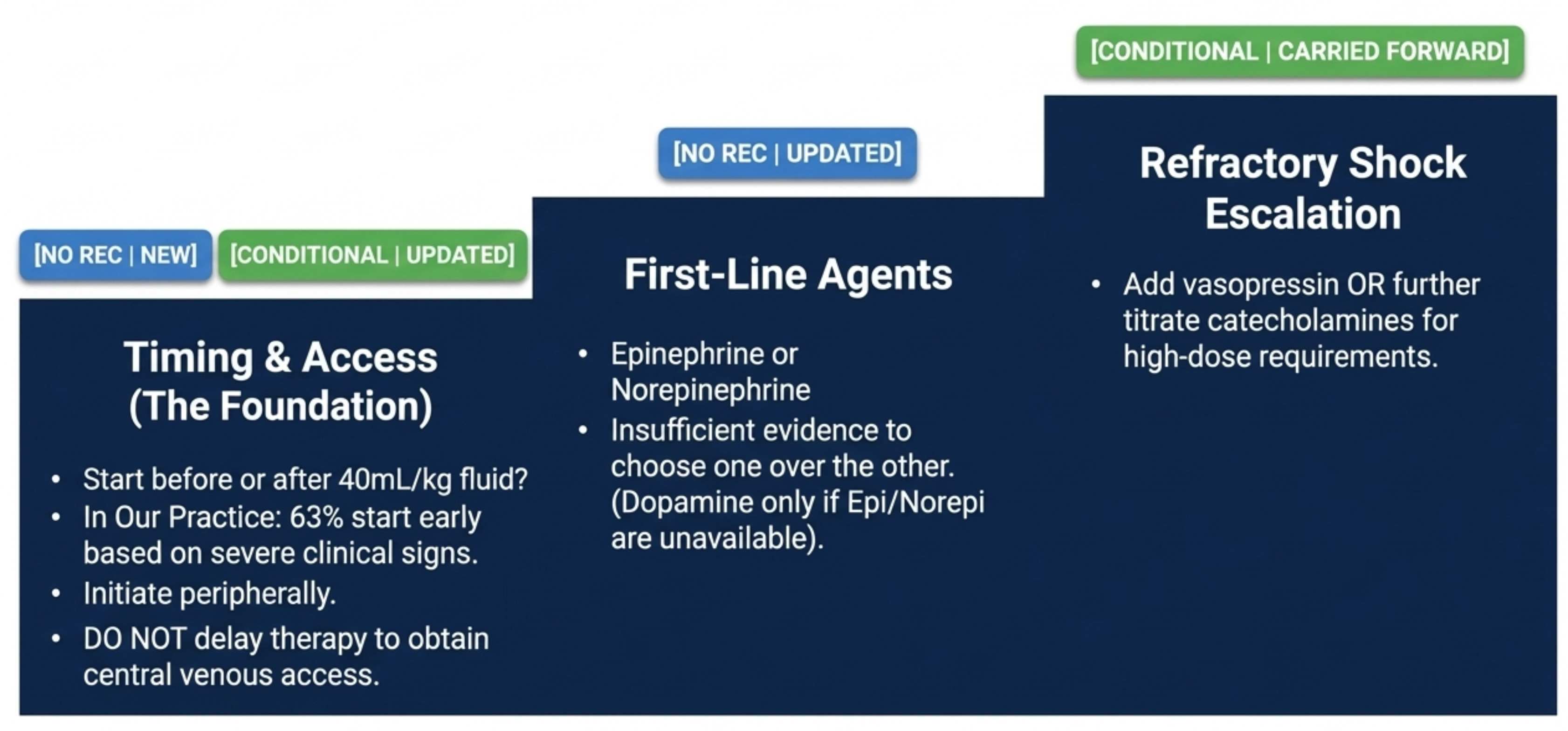
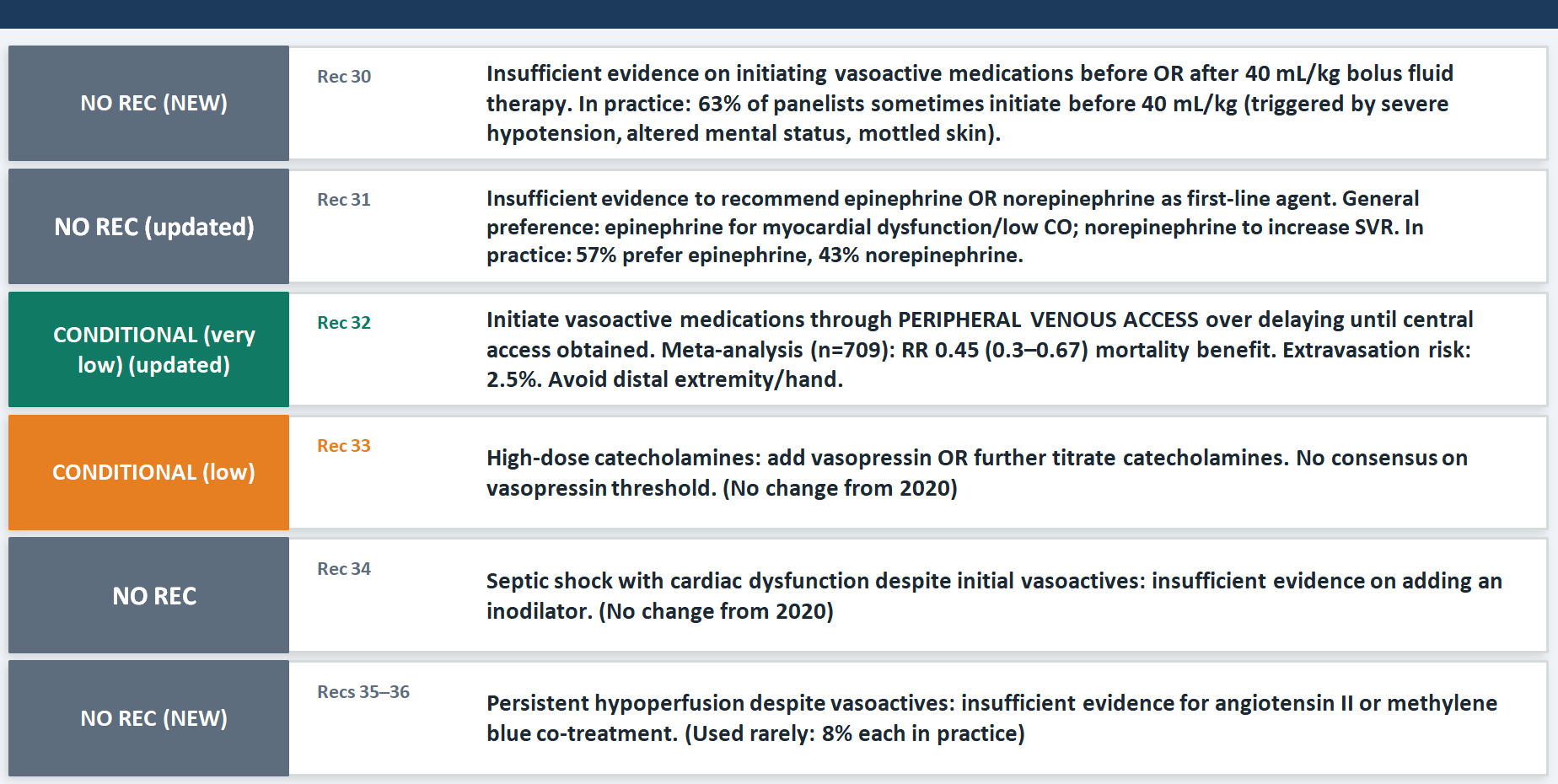
Vasoactive Medications
Two paradigm shifts stand out. The first is the shift on timing: there is now no recommendation either for or against starting vasoactives before 40 mL/kg of fluid (Rec 30), which dissolves the old "fluid first, then pressors" dogma. The emerging pilot data suggest early vasopressors may reduce overall fluid administration — which itself may reduce fluid overload harm. The second shift is the strong conditional recommendation to use peripheral venous access for vasoactives rather than waiting for central access (Rec 32), with a meta-analytic mortality benefit of RR 0.45 and an extravasation risk of only 2.5%. The practical teaching point is that the instinct to wait for central access before starting pressors is costing time that children may not have, especially in the pre-ICU environment.
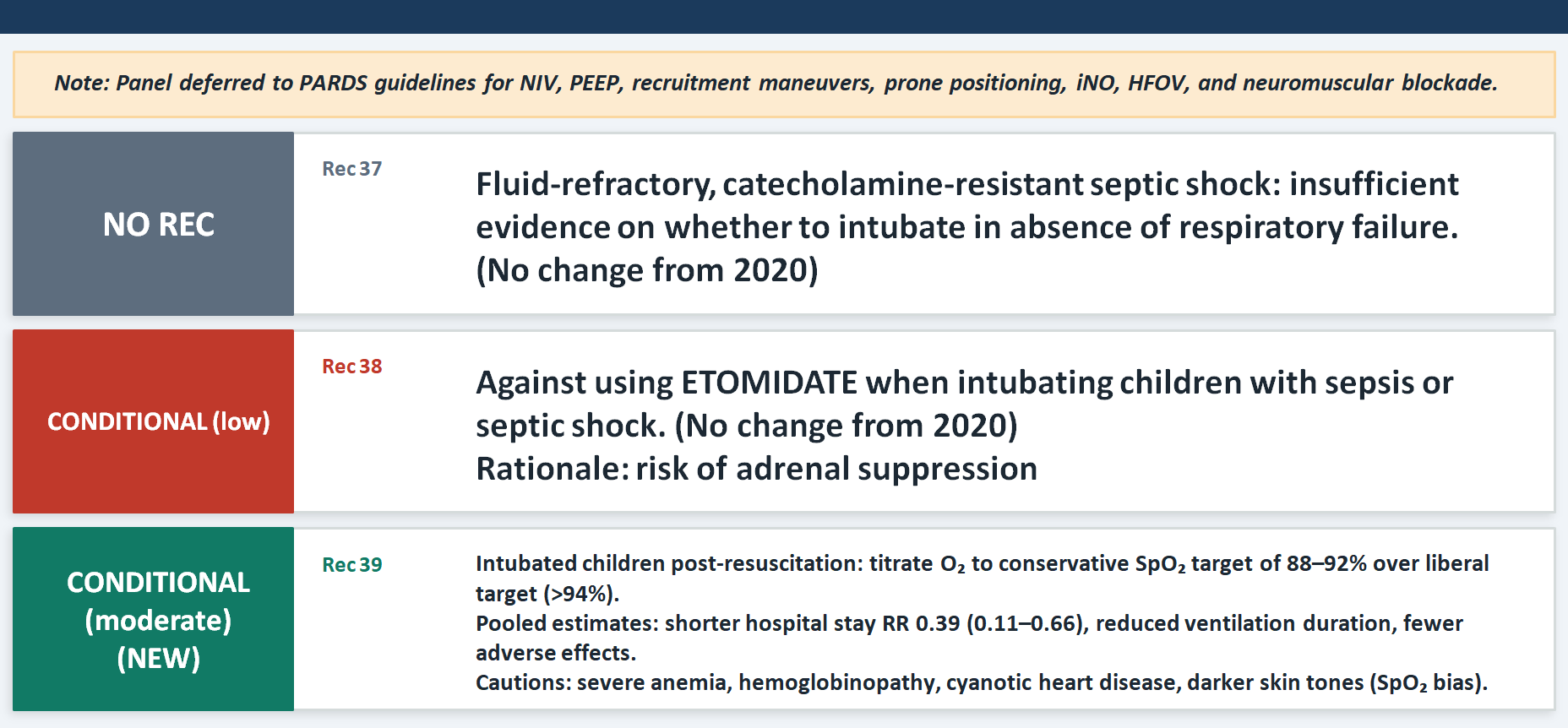
Ventilation
The update here is the new conservative oxygen target: SpO₂ 88–92% over greater than 94% in intubated children after resuscitation (Rec 39, conditional, moderate certainty). This is one of the three moderate/high certainty recommendations and is drawn from the OxyPICU trial and its predecessor data. The physiological logic is important to understand: hyperoxia causes free-radical damage and microcirculatory dysfunction . However, the panel correctly issued only a conditional recommendation because the target should not apply during the acute resuscitation phase, and children with hemoglobinopathies, cyanotic heart disease, or severe anemia may need individualized targets. The note about pulse oximeter bias in darker skin tones is scientifically important.
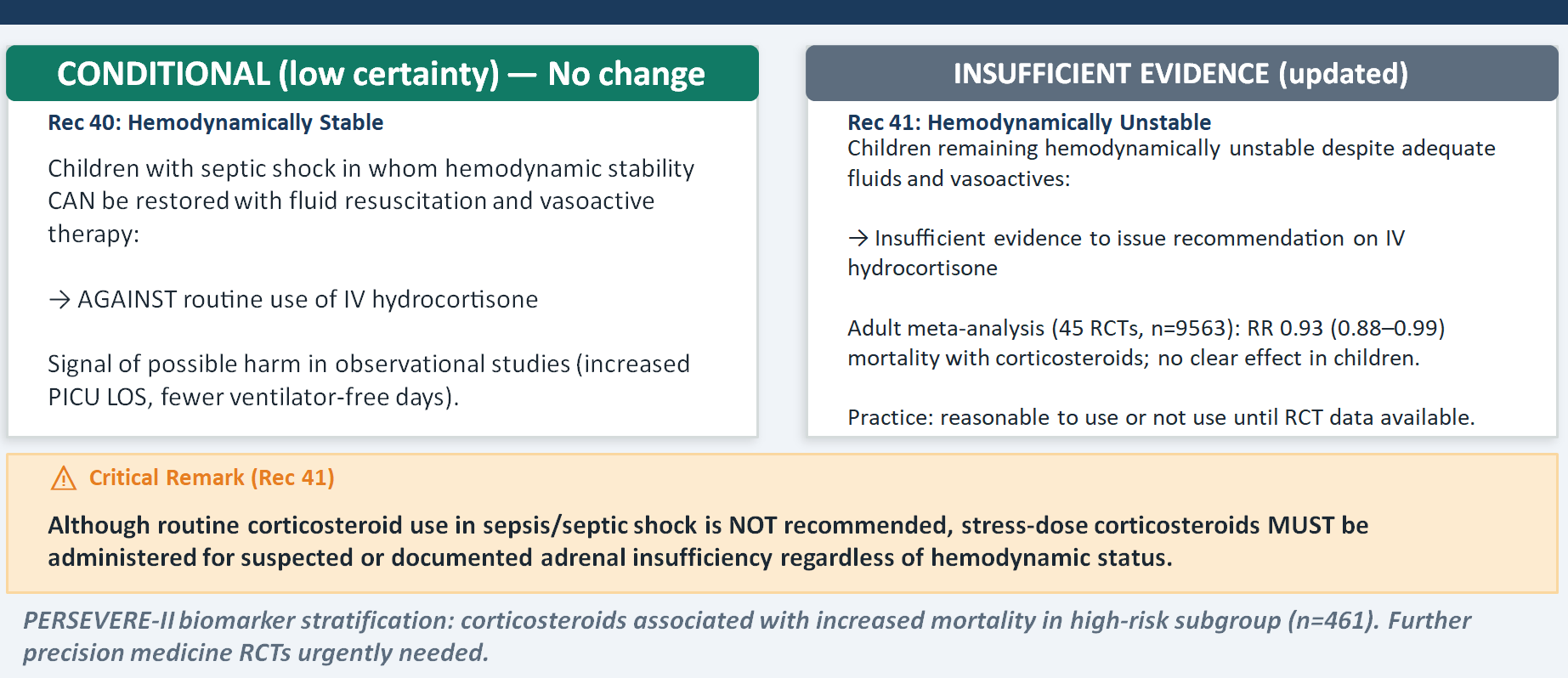
Corticosteroids
Even though the panel could not recommend hydrocortisone for hemodynamically unstable children (insufficient evidence), stress-dose corticosteroids must be given for suspected or documented adrenal insufficiency regardless of hemodynamic status. These are different clinical situations and conflating them causes harm in both directions — over-prescribing in ordinary shock and under-prescribing in relative adrenal insufficiency. The retreat from the 2020 "either/or" language for unstable shock reflects new observational data suggesting possible harm from corticosteroids in children — including longer PICU stays, fewer ventilator-free days, and in biomarker-stratified analyses, increased mortality in high-PERSEVERE-II-score patients. The evidence base here is still weak, but the signal is worrying enough to have updated the language.
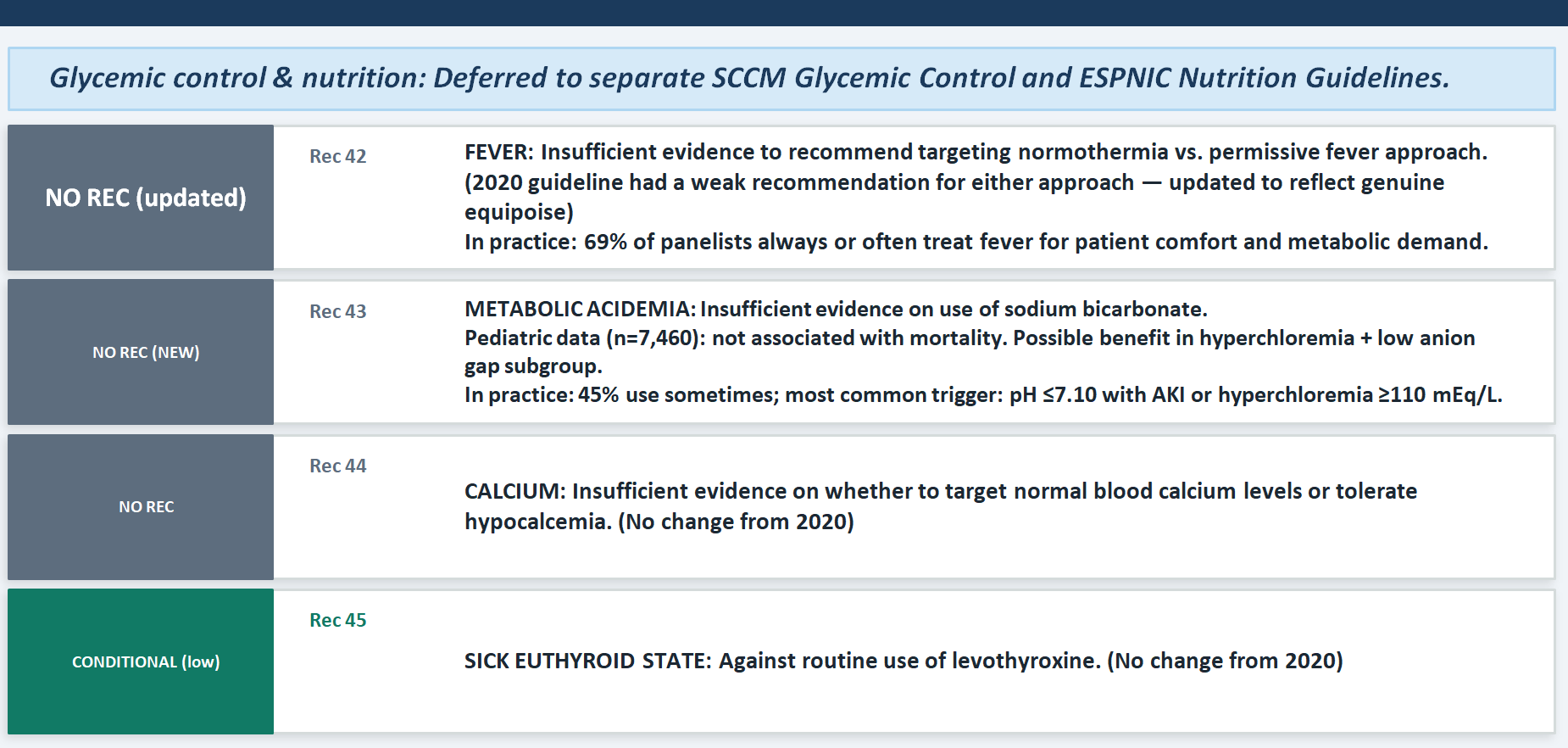
Endocrine, Metabolic & Nutrition
The most important conceptual update is what happened to the fever recommendation: the 2020 guideline had a weak recommendation for either antipyretic therapy or a permissive approach — meaning the panel believed there was enough evidence to gesture toward clinical flexibility. By 2026, even that weak gesture has been withdrawn, replaced by "insufficient evidence." This is a downgrade, and it reflects the genuine equipoise the panel acknowledges: fever has evolutionary survival value (inhibiting pathogen growth, potentiating cellular immunity), but whether that benefit persists in the altered physiology of sepsis is unknown. For sodium bicarbonate in metabolic acidemia (Rec 43, new), the take-home is that the data are truly uncertain — the retrospective pediatric cohort of over 7,000 children showed no overall mortality benefit, with a possible benefit only in the hyperchloremia/low-anion-gap subgroup, suggesting that the biochemical context in which you use bicarbonate matters profoundly.
Vitamins & Supplements
vitamin C (Rec 46), thiamine (Rec 47), and vitamin D (Rec 48) should not be used routinely in pediatric sepsis. The VITACiPS RCT for vitamin C (n=218) and the RESPOND PICU trial for vitamin C + thiamine + hydrocortisone (n=60) both showed no benefit on organ dysfunction, shock reversal, or mortality. What makes this teaching-worthy is not the negative result itself but the important exception the panel preserves: in patients with documented or suspected deficiency — particularly malnourished children — vitamin C and thiamine repletion may still be appropriate. This prevents the guideline from being applied as a blanket prohibition when genuine nutritional deficiency is present.
Fluid Balance, RRT & ECMO
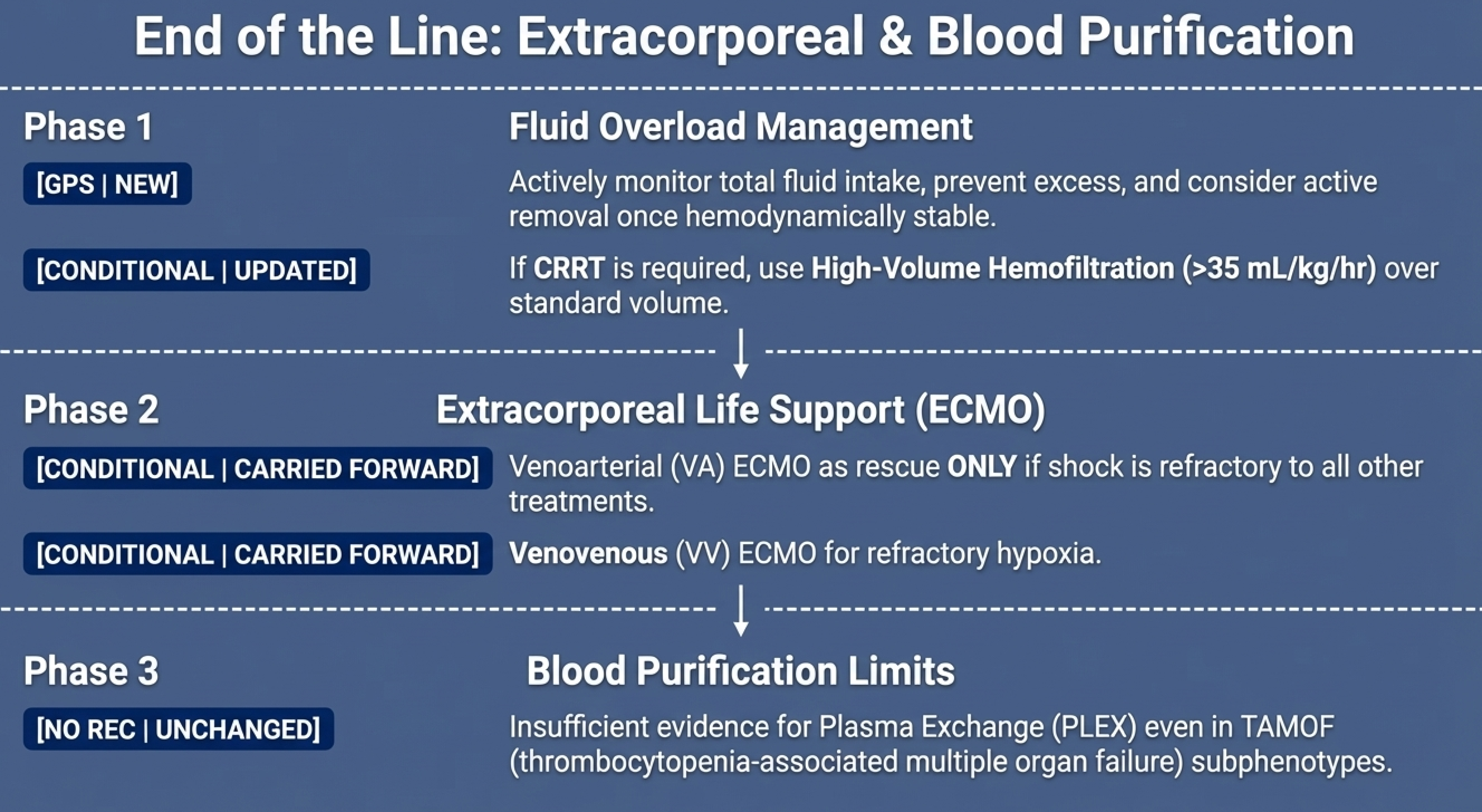
The most significant reversal from 2020 is the HVHF recommendation (Rec 50): the 2020 guidelines suggested against high-volume hemofiltration, while the 2026 guidelines now conditionally recommend it over standard-volume hemofiltration. The new meta-analysis of three RCTs (n=195) shows a mortality benefit (RR 0.58) and shorter RRT duration. However, students and practitioners should understand the caveats: all three trials used continuous venovenous hemofiltration (CVVH) specifically, the evidence base is still small, and this is only applicable where CRRT infrastructure exists. The GPS on fluid overload management (Rec 49) is architecturally important: it frames fluid removal as a proactive strategy once hemodynamic stability is achieved, not a reactive crisis measure — and 64% of panelists already do this in practice.
Immune Therapies
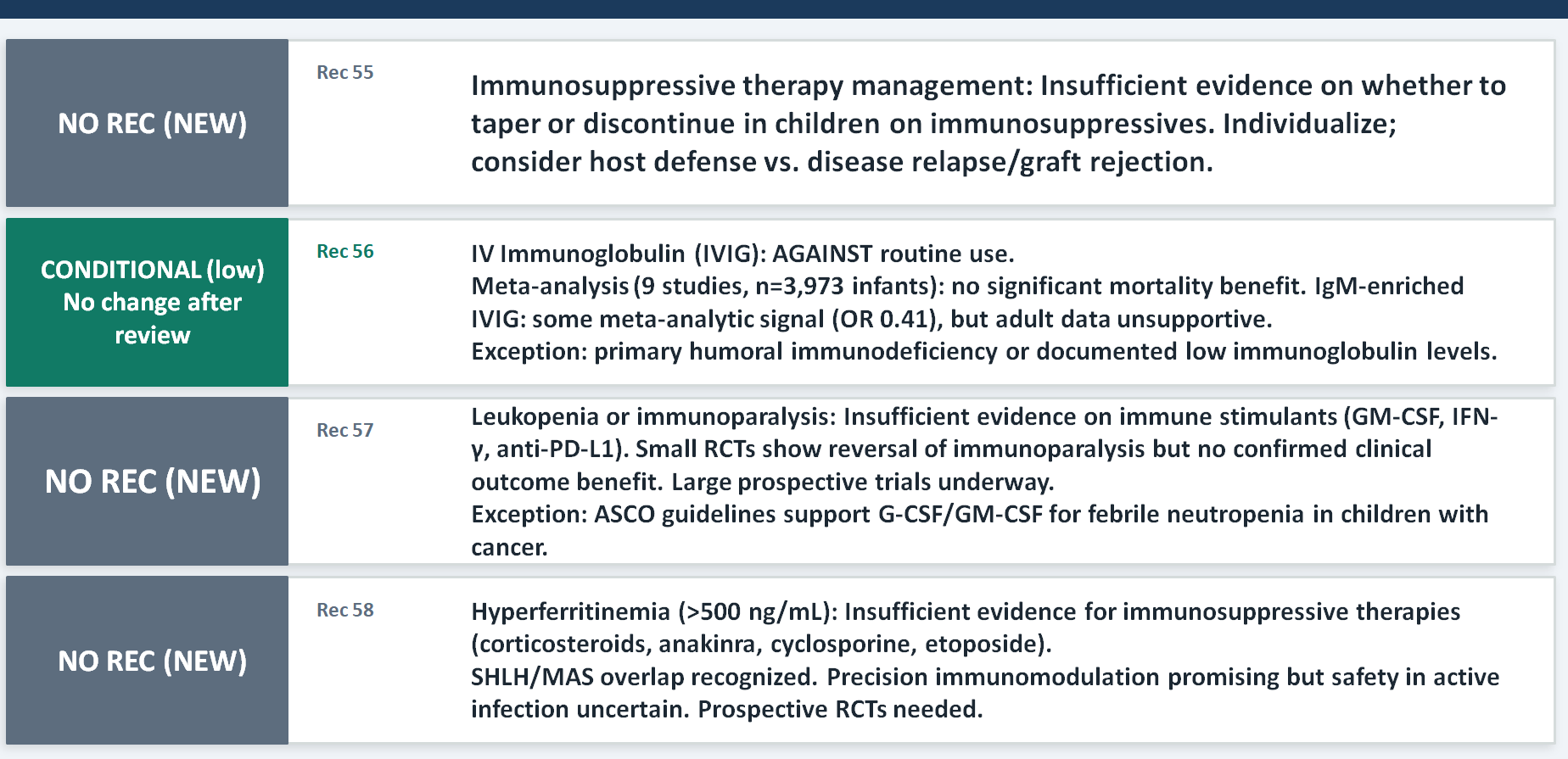
The section on hyperferritinemia (Rec 58) is the most intellectually exciting new addition in this domain. It represents the field beginning to grapple with precision immunomodulation — the recognition that sepsis is not immunologically uniform, and that children with features of secondary HLH, macrophage activation syndrome, or cytokine storm may need immune suppression rather than immune stimulation. But the panel is appropriately cautious: most data come from non-sepsis populations (rheumatologic disease, malignancy), and the safety of immunosuppression in children with active infection and heterogeneous immune competence remains uncertain. The IVIG recommendation (Rec 56) reinforces a consistent message across guidelines: no routine use, but consider it in children with primary humoral immunodeficiency or documented low immunoglobulin levels.
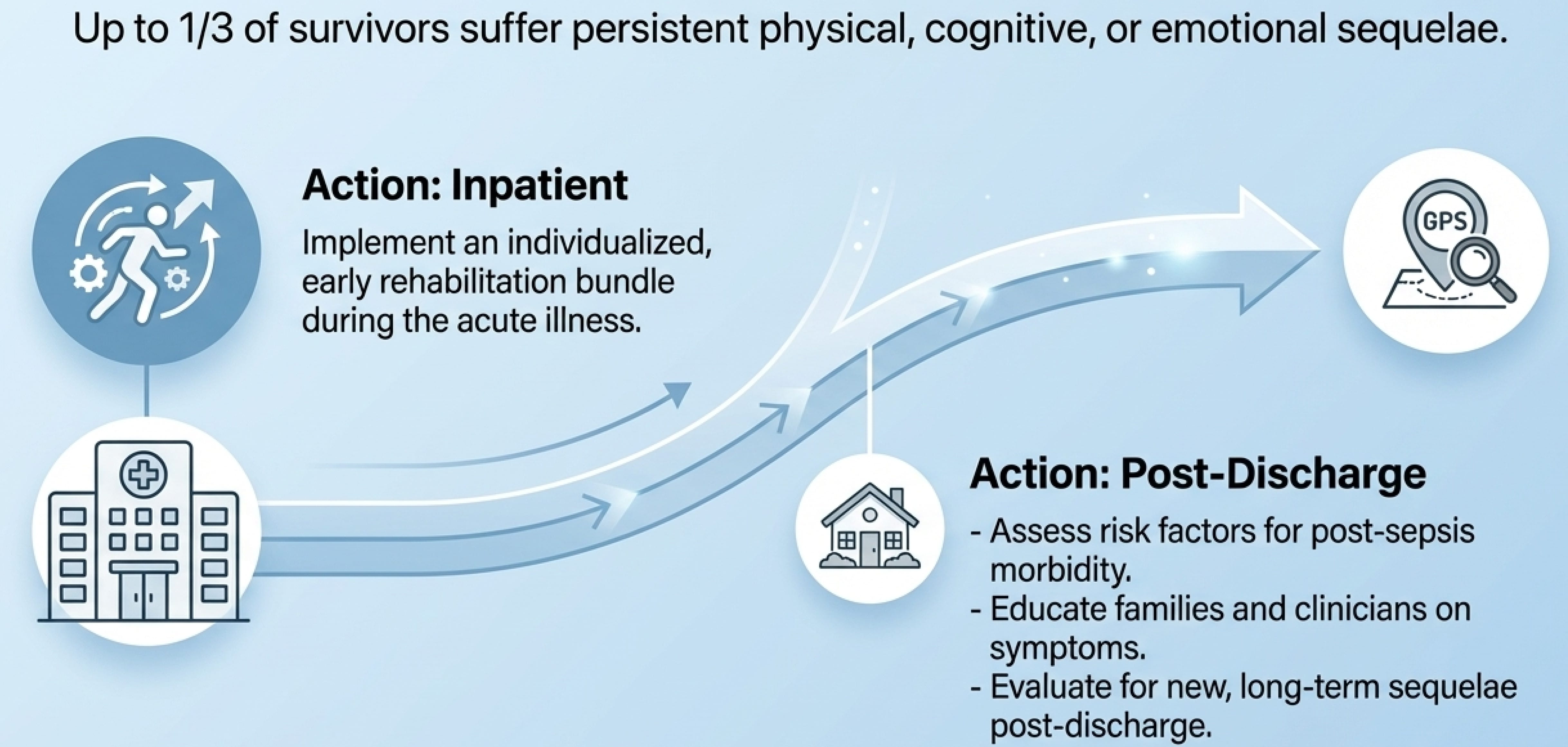
Long-term Follow-up
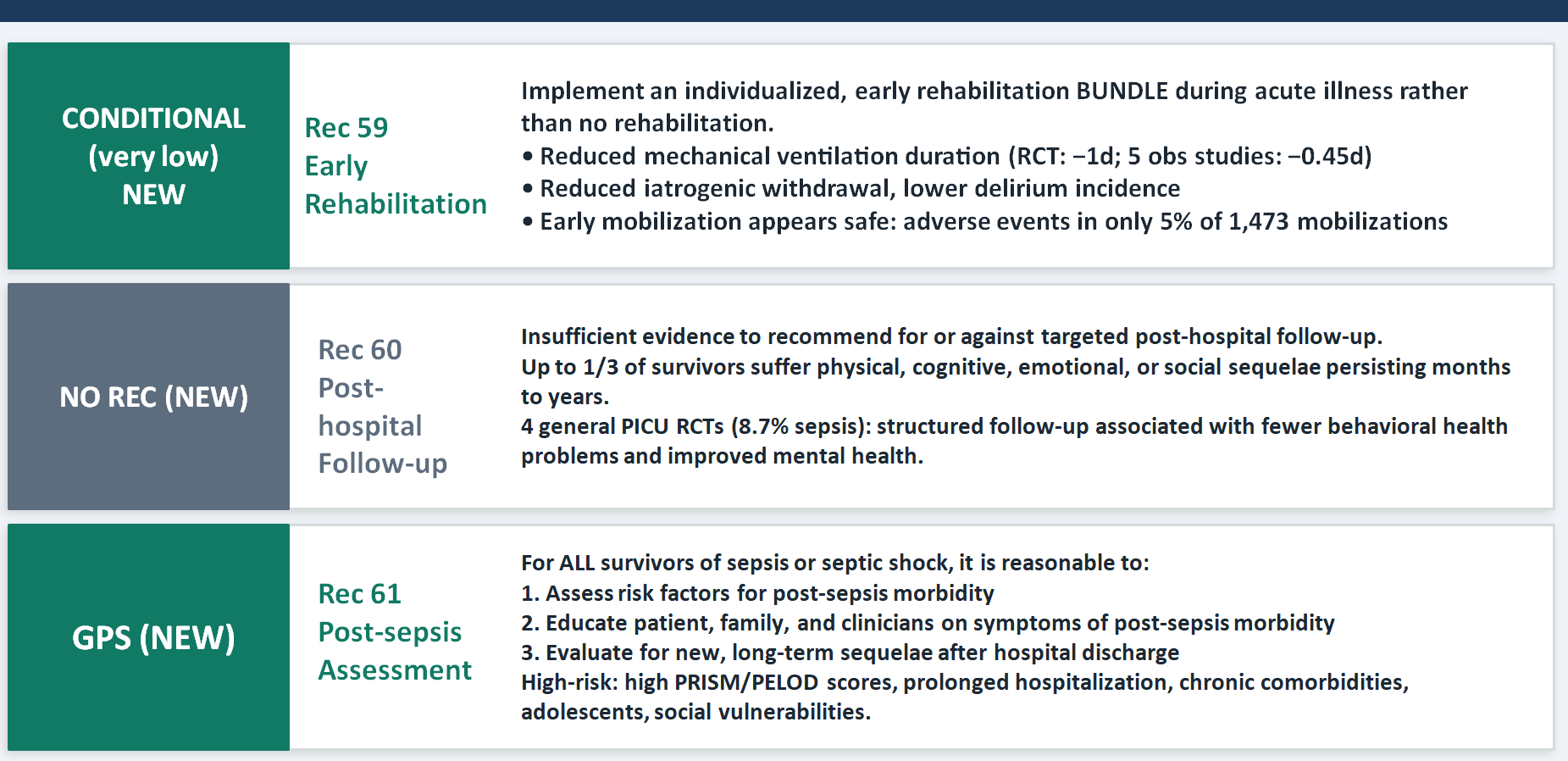
This is the most conceptually new section in the entire guideline update, and its message is almost philosophical: surviving sepsis is not the endpoint of care, it is a waypoint. Up to one-third of survivors carry physical, cognitive, emotional, or social sequelae for months to years. The early rehabilitation bundle recommendation (Rec 59) is actionable now — it includes reducing sedation, preventing delirium, promoting sleep, facilitating early ventilator liberation, and engaging families. The GPS for post-sepsis assessment (Rec 61) creates a professional obligation: screen for risk factors, educate families, and evaluate for long-term sequelae after discharge. The practical teaching point is that pediatric intensivists and emergency physicians must see their role as extending beyond the ICU walls — and that the family, not just the child, is the unit of care.
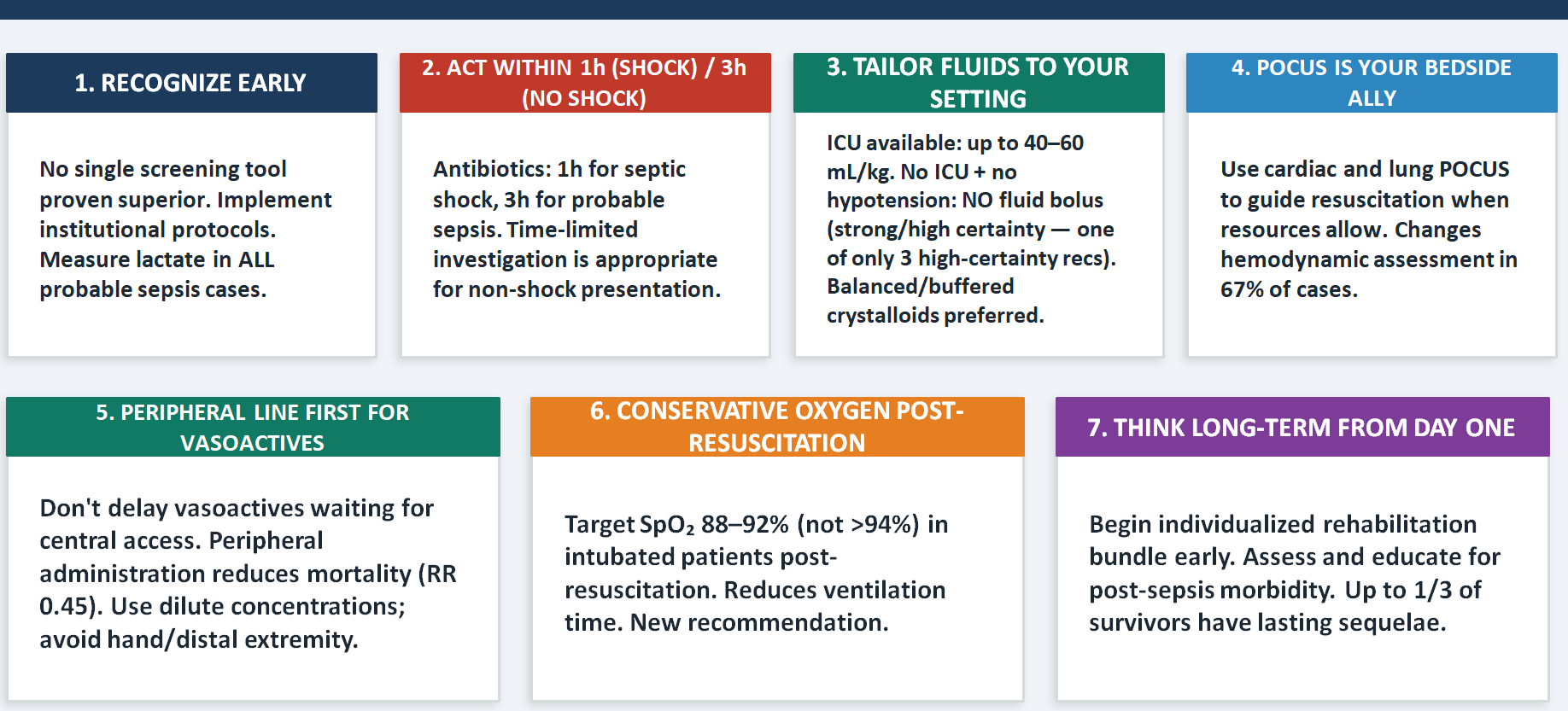
Key Clinical takeaways
Each of the seven pearls represents a node where the guideline either changed practice or reinforced it with new evidence. The most counterintuitive three — worth specifically teaching — are the retreat from universal screening, the embrace of peripheral access for vasoactives, and the conservative SpO₂ target of 88–92%. These three challenge instincts that have been deeply embedded in training for decades.
The fluid tailoring message is particularly important for low-resource settings like India, where the strong recommendation against fluid boluses in the absence of hypotension without ICU backup has enormous population-level implications. And the long-term follow-up pearl is arguably the most humanistic message in the entire deck: the child who walks out of the PICU carries the sepsis with them.
These guidelines are a general scheme of care, not a treatment algorithm. They cannot account for the individual child in front of you, your local pathogen ecology, your resource constraints, or the family's values and preferences. The panel says this explicitly, repeatedly.
The closing message is one of intellectual humility: even 68 world experts working with the best available evidence can only gesture toward the right answer in most clinical situations. Clinical judgment, informed by these guidelines but not replaced by them, remains the irreducible core of good medicine.
Further reading: Weiss SL, Peters MJ, Oczkowski SJW, et al. Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026. Intensive Care Med. Published online March 23, 2026. doi:10.1007/s00134-026-08360-2