Cardiometabolic multiple long-term conditions (MLTC)
Understand by pictures ....

Cardiometabolic multiple long-term conditions (MLTC), defined as the coexistence of two or more cardiometabolic diseases such as diabetes, cardiovascular disease, and chronic kidney disease, are increasingly prevalent and represent a growing challenge for health systems worldwide.
The growing number of people living with multiple long-term conditions (MLTC) is one of the defining challenges facing health care globally.Research in this field has challenged the single-disease framework that has traditionally dominated service design and research focus. But progress in MLTC research has been hampered by methodological inconsistency, definitional imprecision, and the difficulty of designing effective interventions for highly heterogeneous MLTC populations. These limitations have prompted calls to shift focus to narrower and potentially more tractable common clusters of conditions with a disproportionate impact on outcomes such as mortality, quality of life, and health service use.
Evolution of terminology of multimorbidity
•The term multimorbidity was first described by Brandlmeier in an urban German general practice in 1976.
•In view of the confusion in terminologies between comorbidity and multimorbidity, a distinction was proposed in 1996 with the term comorbidity implying combined effects in reference to an index chronic condition (eg, stroke in a person with diabetes) and multimorbidity meaning co-occurrence of conditions without a single condition holding a priority over other co-occuring conditions.
•The concept of multimorbidity as two or more chronic conditions was adopted by WHO in 2008 in recognition of its growing burden in an ageing society.
•In 2018, the Academy of Medical Sciences published a landmark international policy report titled Multimorbidity: a priority for global health research. The report highlighted the rising burden of multiple long-term conditions and the lack of coherent evidence on its causes, prevention, and management.
•Patients do not find multimorbidity an acceptable term to describe their condition and associate it with a negative image, giving the impression to patients that they are in poor health, their body is failing them, they may be dying soon, and there is nothing they can do about their condition. The UK National Institute for Health and Care Research Strategic Framework therefore emphasised their preferred term as multiple long-term conditions.
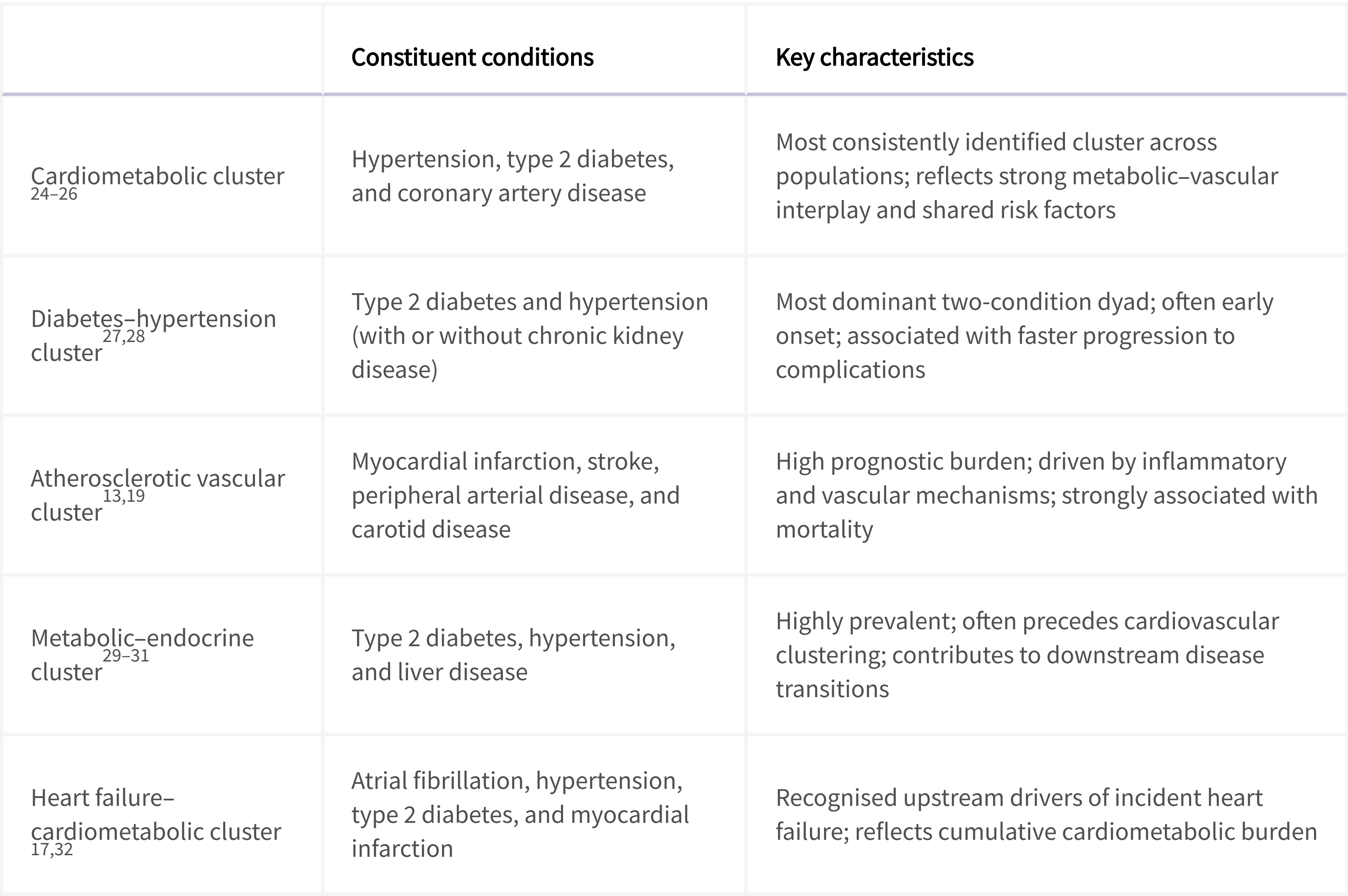
Cardiometabolic conditions most strongly contributing to observed cardiometabolic multiple long-term condition clusters
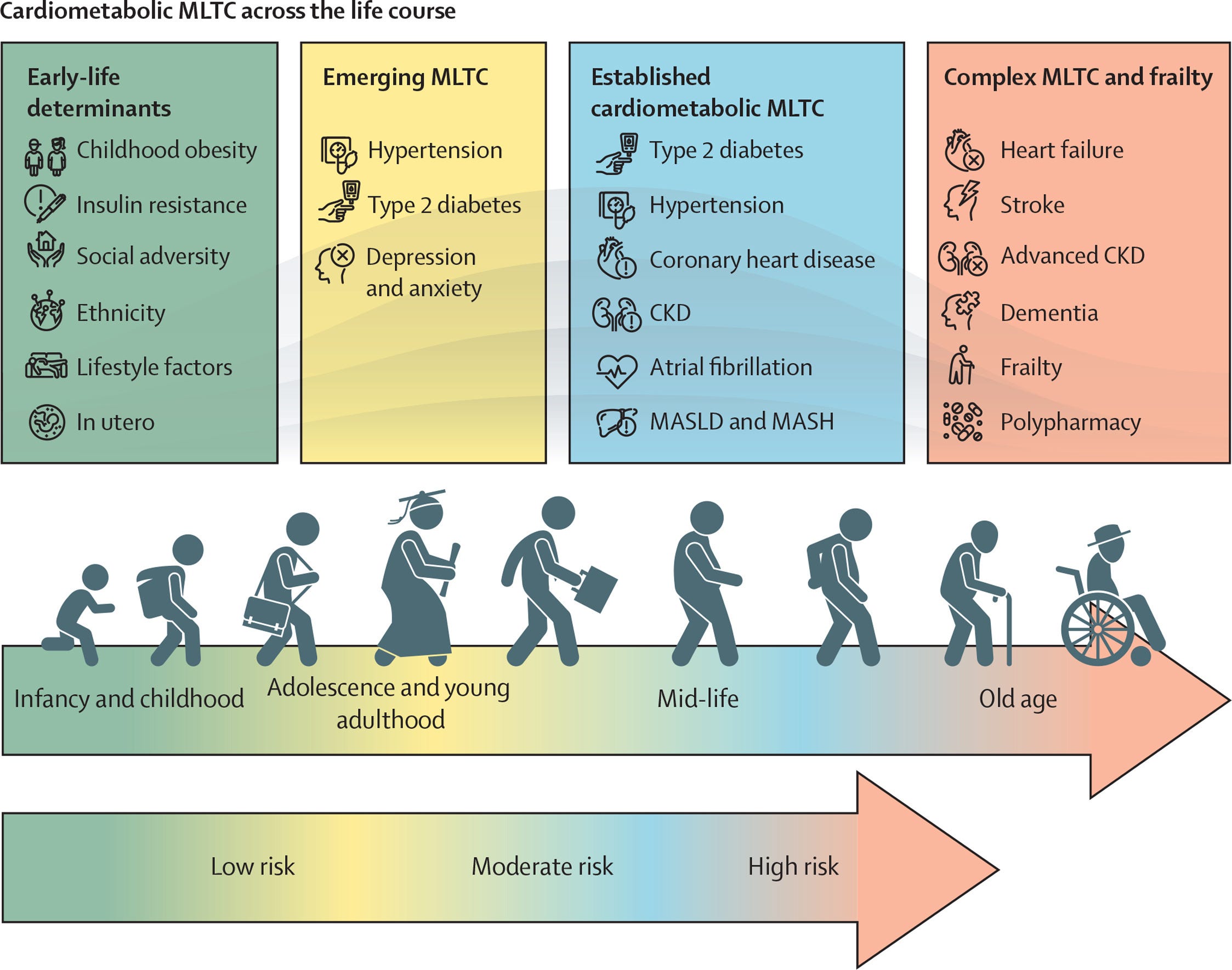
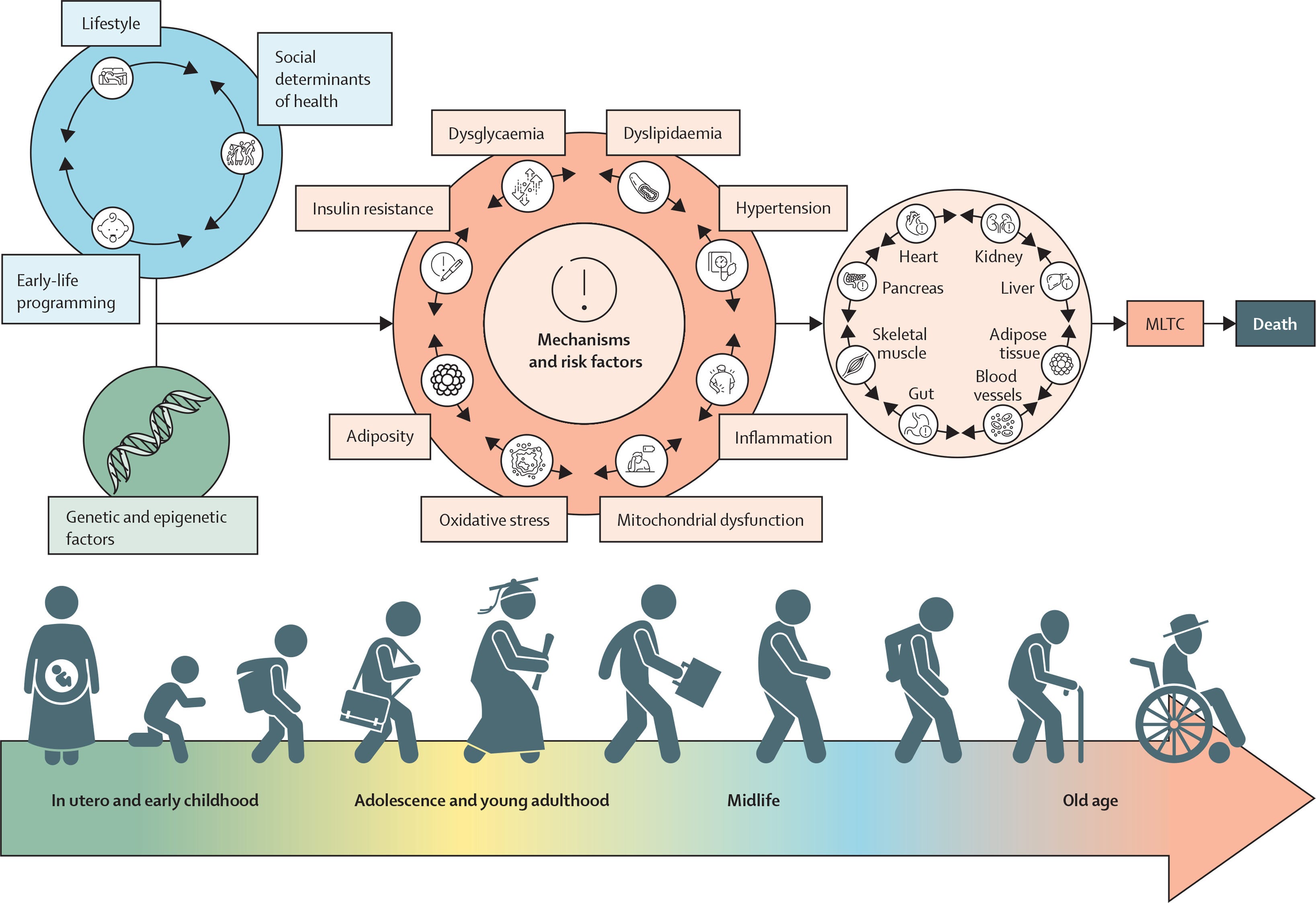
MLTC across the life course
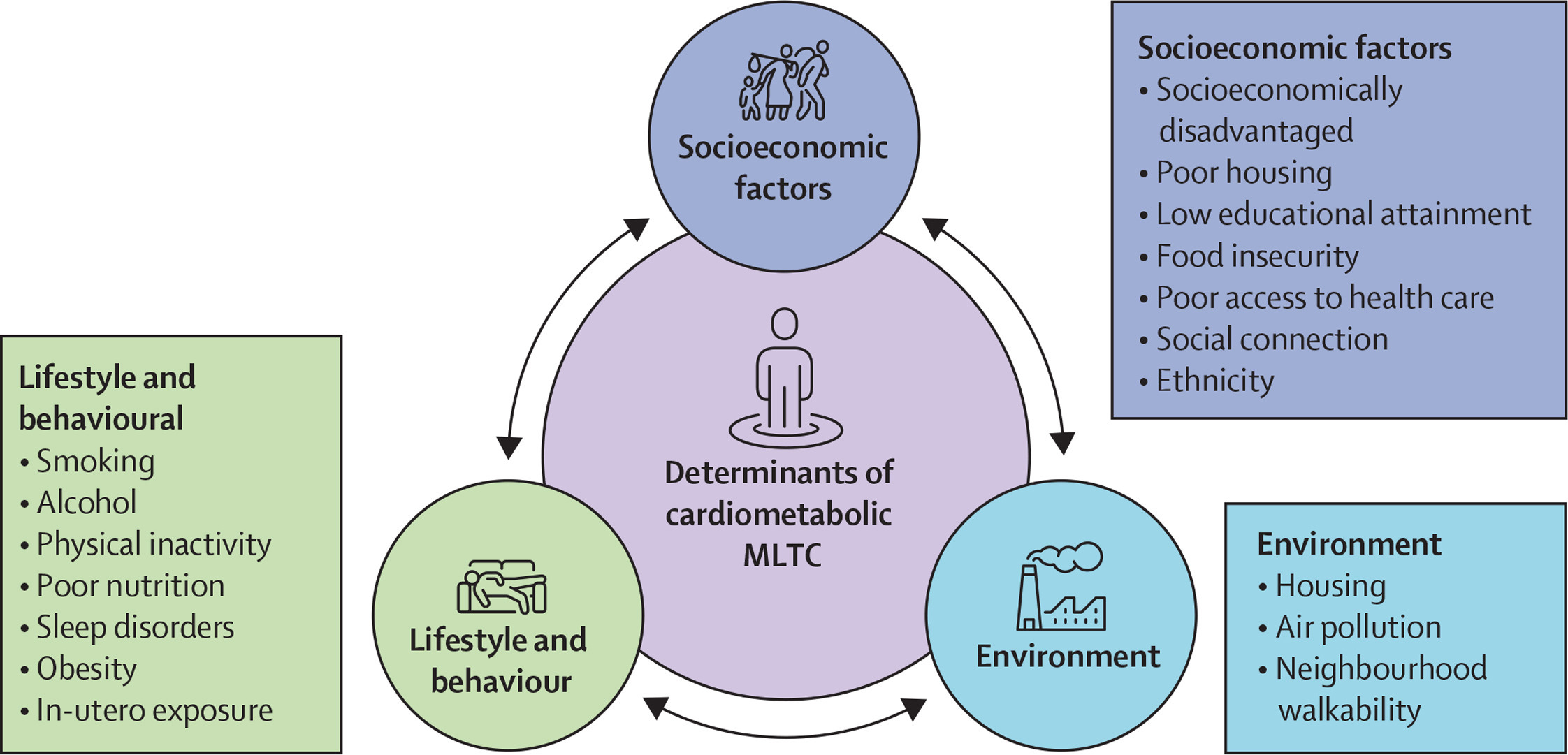
Determinants of cardiometabolic MLTC
Cardiometabolic MLTC arise from a complex interplay of biological, behavioural, social, and environmental determinants; genetic susceptibility; metabolic pathways; ageing; adiposity; insulin resistance; and chronic inflammation, with some determinants being modifiable . One genome-wide association study showed that there are 11 independent genetic variants associated with psycho-cardiometabolic MLTC, with a polygenic risk score being predictive of co-occurrence of depression, coronary artery disease, and type 2 diabetes, and suggested eight causal factors (BMI, body fat percentage, LDL cholesterol, total cholesterol, fasting insulin, income, insomnia, and childhood maltreatment).
The sequencing of conditions and effect on outcomes
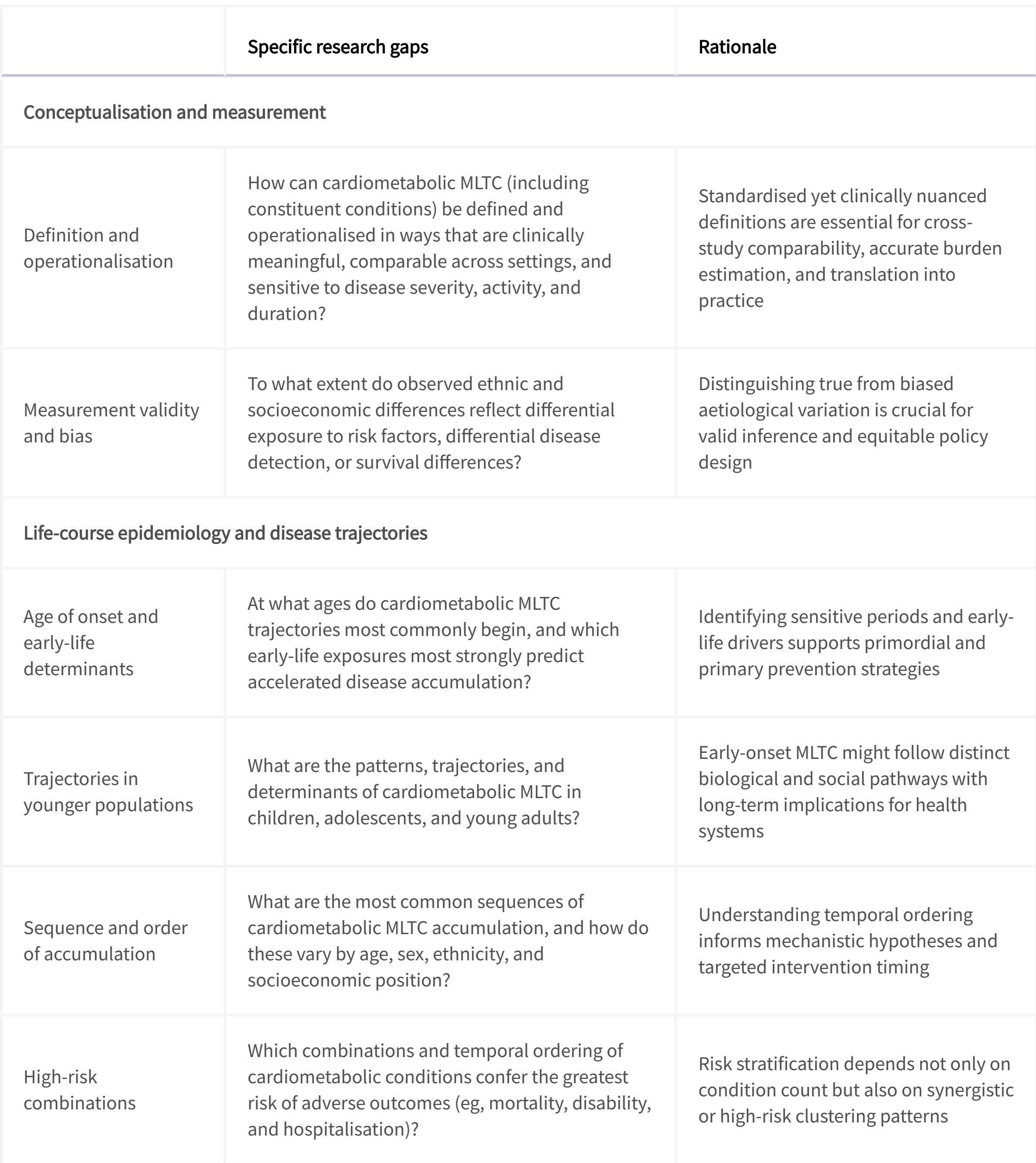
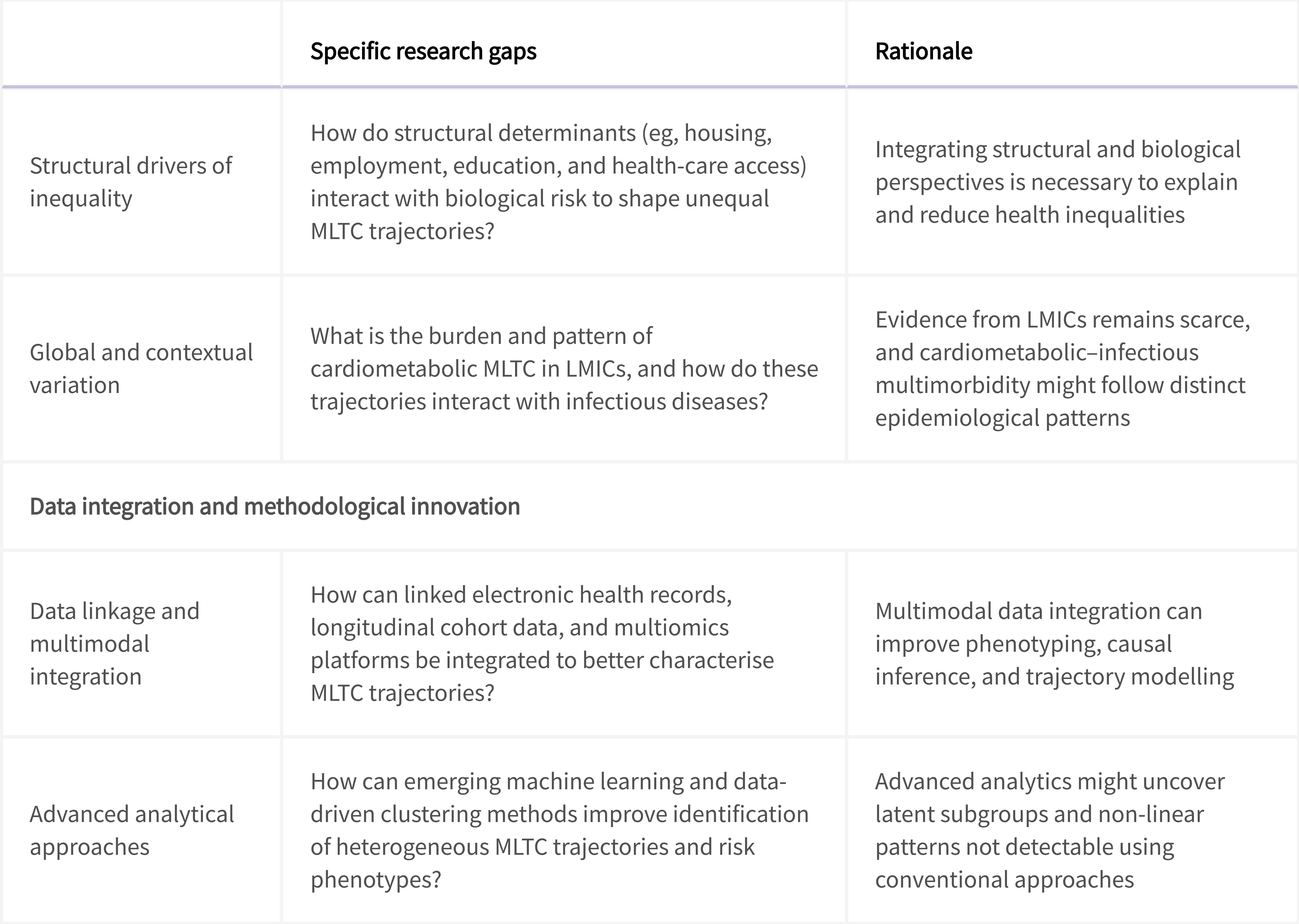
Methodological challenges and future research gaps

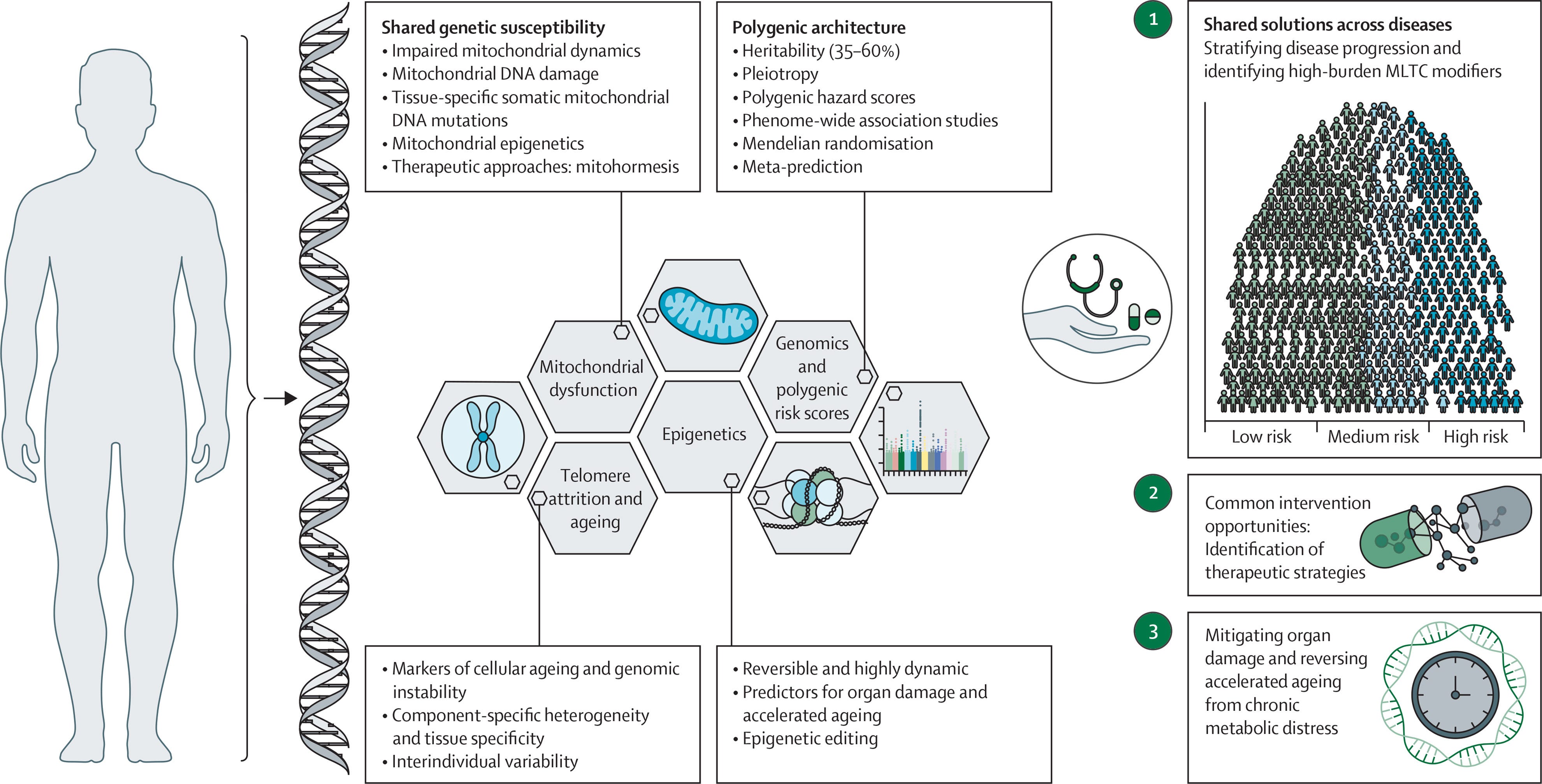
Biological and mechanistic pathways of cardiometabolic multiple long-term conditions
Role of genetic and epigenetic biomarkers
Interventions for the prevention and management of cardiometabolic multiple long-term conditions
Multifaceted approach to cardiometabolic MLTC
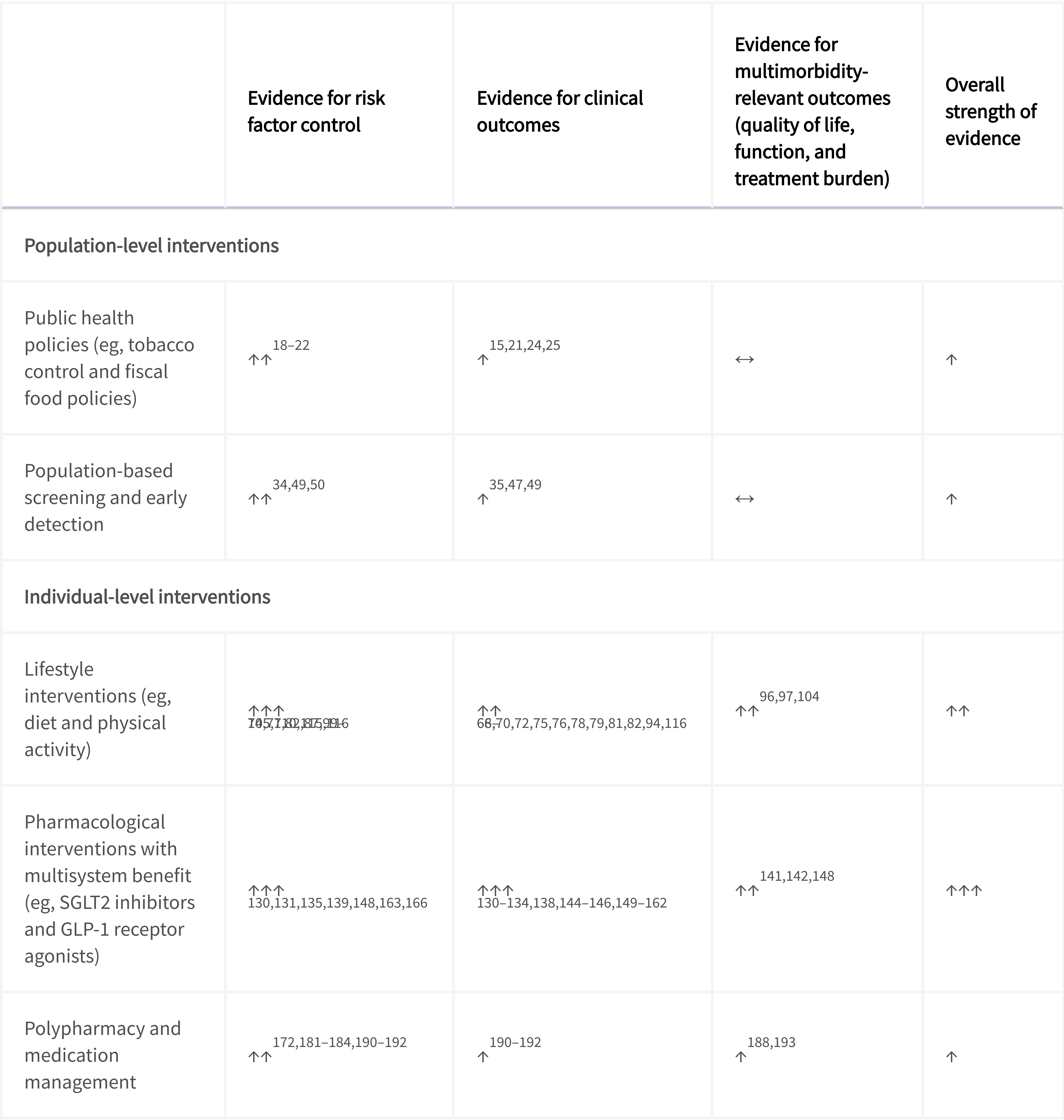
Evidence base for prevention and management interventions in cardiometabolic multiple long-term conditions
Key research gaps
Population-level interventions
•High-quality evaluations using real-world data, rather than modelling studies, are needed for assessing the effect of population-level interventions on the prevention and management of cardiometabolic multiple long-term conditions (MLTC).
•There is limited evidence on populations at high risk, such as those from socioeconomically deprived areas and minority ethnic communities.
•Most studies have been in older populations and further research is needed for younger populations who are facing a growing burden of MLTC.
•There is a scarcity of high-quality trials in low-income and middle-income countries.
Individual-level interventions
•Clarity is required as to what are the most meaningful primary endpoints for intervention trials in individuals with, or at risk of, cardiometabolic MLTC.
•There is insufficient high-quality evidence that in-person behavioural interventions in people with cardiometabolic MLTC produce sustained improvements in risk factor control and cardiometabolic outcomes.
•Evidence for digital and artificial intelligence-based delivery of lifestyle interventions to improve clinical outcomes and address health inequalities remains scarce.
•Evidence is needed to understand optimal timing and intensity of treatment with novel pharmacotherapies in different risk groups across the life course in cardiometabolic MLTC.
•Further evidence is required to understand the effect of rational polypharmacy and deprescribing on clinical outcomes in cardiometabolic MLTC across the life course.
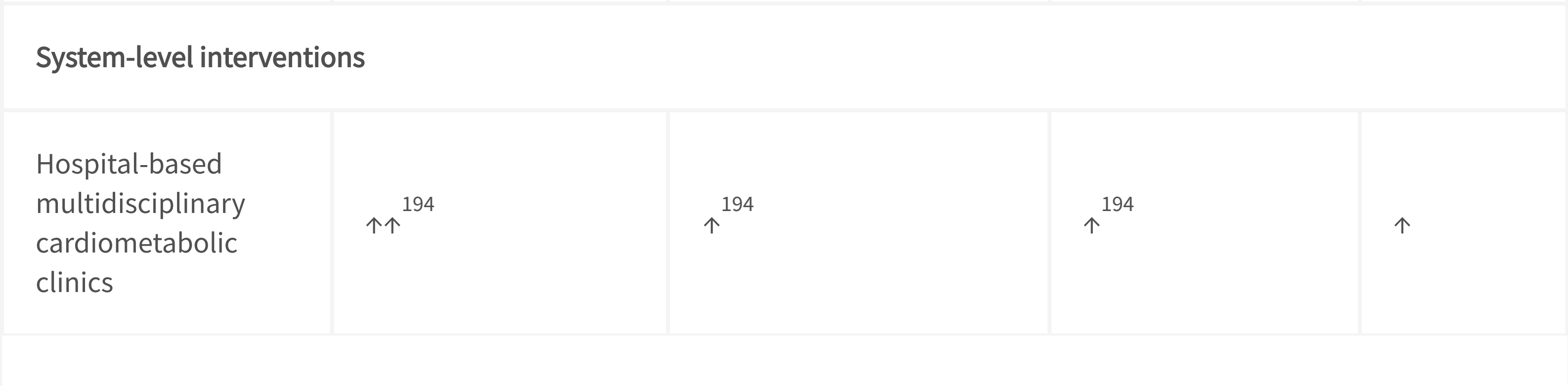
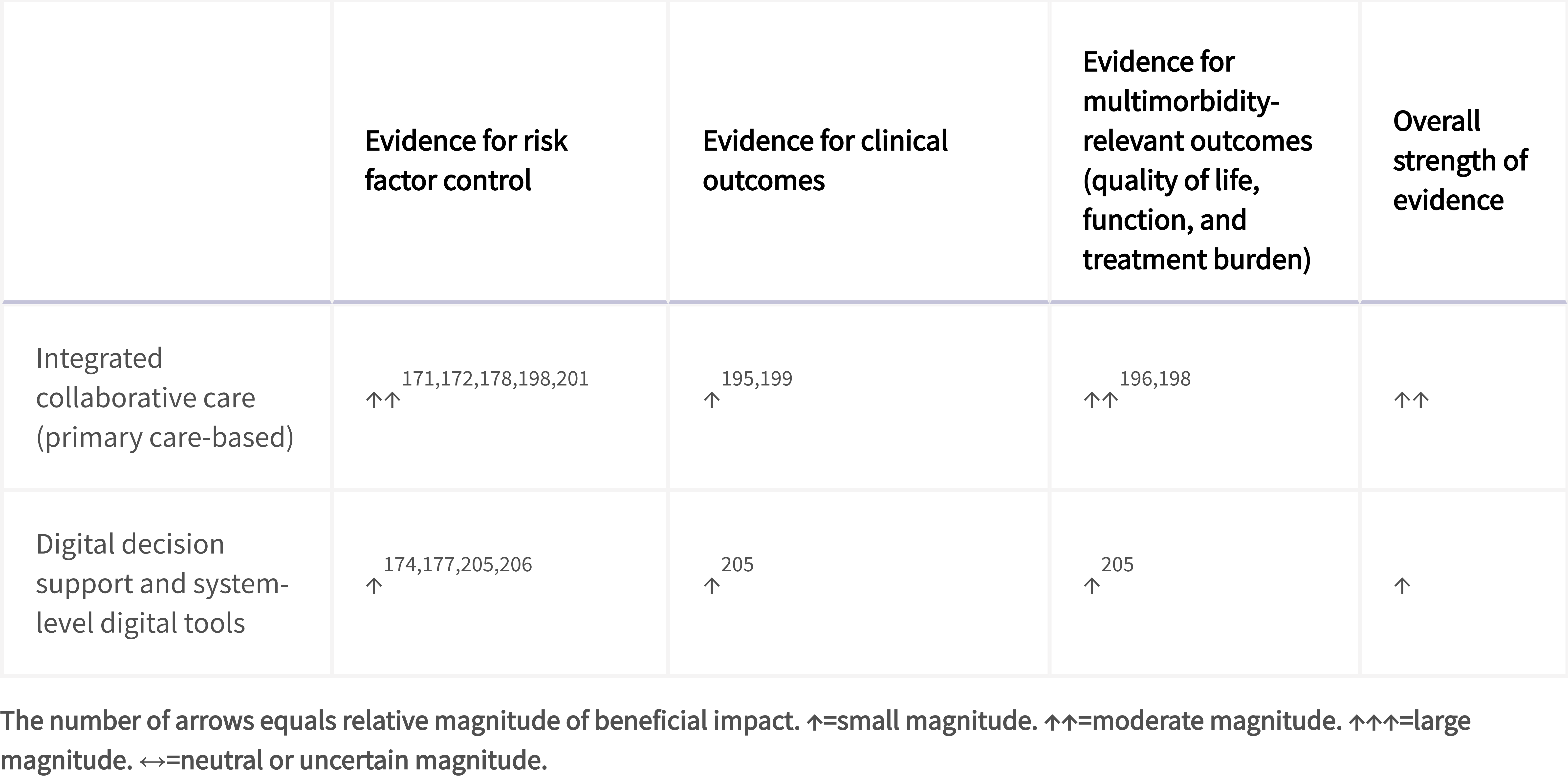
System-level interventions
•Further research is required on pragmatic models of care for improving outcomes of people with established cardiometabolic MLTC.
•There is a lack of multimorbidity-specific outcomes, with most studies prioritising single behaviours or conditions rather than outcomes relevant to MLTC (eg, treatment burden, functional status, or integrated risk reduction).
•Future studies should include complex interventions integrating behavioural interventions, digital tools, care coordination, and health system infrastructure.
•Evidence for system-level digital interventions, including artificial intelligence and large language model-enabled decision-support systems, remains scarce.
Key evidence gaps and future research priorities in cardiometabolic MLTC
Shared risk factors and mechanisms
•Identify shared causal molecular pathways for therapeutic targeting
•Delineate the neuroendocrine–immune axes that drive the development of cardiometabolic multiple long-term conditions (MLTC)
•Delineate the temporal stages in the evolution of cardiometabolic MLTC to identify critical windows for intervention
SDOH
•Standardise consensus-based criteria for the uniform definition of social determinants of health (SDOH) and objective measurements of cardiometabolic MLTC and disease severity
•Broaden the scope of SDOH by capturing socioeconomic, environmental, behavioural, and structural factors (eg, social support, housing quality, and neighbourhood safety) using standardised instruments
•Investigate the link between SDOH and cardiometabolic MLTC by conducting prospective real-world studies in diverse populations, including in marginalised groups and different health-care settings
Early-life exposures and programming
•Delineate the mechanisms by which early-life exposures alter the composition and functions of the gut microbiome
•Define the window-specific contribution of different developmental periods, from preconception, in utero, infancy, and adolescence to the final risk of cardiometabolic MLTC
•Analyse longitudinal trajectories for determining the crucial transition point at which cardiovascular and metabolic risk factors solidify into cardiometabolic MLTC
Genetic and epigenetic biomarkers
•Identify genetic modifiers within high-burden cardiometabolic MLTC, such as cardiovascular–kidney–liver–metabolic conditions
•Identify possible rare and structural variants and characterise their contributions to account for missing heritability
•Determine the relative influence of genetic, phenotypic, and environmental crosstalks on interindividual differences in MLTC progression
•Determine the cell-specific, persistent epigenetic changes (eg, DNA methylation and histone modifications in adipocytes or endothelial cells) that explain the effect of early-life exposures
•Measure and validate mitochondrial damage and dynamics markers (eg, cell-free mitochondrial DNA and key metabolites) in ethnically diverse cohorts
Emerging non-genetic biomarkers
•Integrate multiomics data for the discovery of novel, cross-disease biomarkers for improved risk stratification, prediction, and prognostication of cardiometabolic MLTC
•Validate multiomics signatures that can predict the transition from a single disease to cardiometabolic MLTC and the disease trajectories
•Delineate circulating molecular ageing markers that can predict and mediate inflammation-driven organ damage across various tissues
Further reading:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00606-9/fulltext
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)01078-0/fulltext
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00607-0/fulltext
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00608-2/fulltext