All in One Case
A Human Body Can Fail Without Warning. A Healthcare System Should Not.

Yesterday, I was sitting with a colleague when his phone rang. He stepped away from the table. When he returned, something had changed in his face. His eyes were wet. His expression had that stillness one sees in people who have just heard news that the mind has not yet absorbed.
I did not ask immediately.
In medicine, some silences arrive already diagnosed.
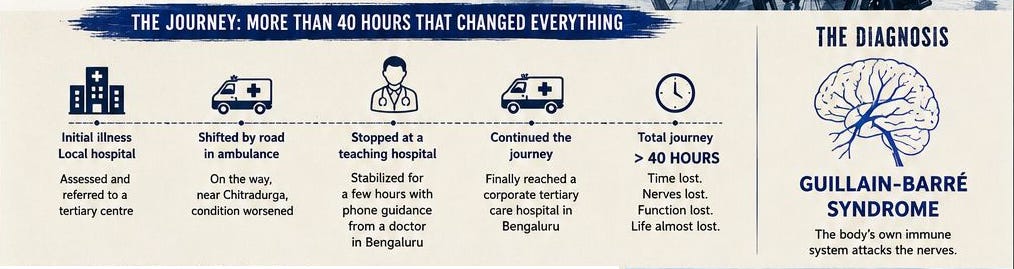
After a few moments, he told me the story. His biology professor from his pre-university college days had called him from far away. He was 65 years old now. A year earlier, this man had still been teaching biology to pre-university students. He was working, explaining life to young minds, using his voice, his hands, his memory, his body, and his years of accumulated confidence in the classroom. Then came an illness that began as weakness and later acquired a name: Guillain-Barré syndrome.
The name is tidy. The disease is not…!
On paper, Guillain-Barré syndrome is an acute immune-mediated neuropathy, often triggered after an infection, in which the body’s immune system attacks peripheral nerves. In real life, it can be a terrifying betrayal. A person who was walking, speaking, swallowing, eating, teaching and breathing normally may, over days, begin to lose the ordinary functions that make life feel secure. Legs fail. Hands weaken. Voice changes. Swallowing becomes unsafe. Breathing, that quiet background rhythm of existence, becomes an excessive work...!
We speak of “ascending paralysis” in textbooks. But no family experiences it as a phrase. They experience it as panic moving upward.
The family first took him to a local hospital. The doctor there assessed him and referred him to a tertiary care hospital in Bengaluru. The patient was shifted by road in an ambulance. Somewhere on the way, near Chitradurga, his condition worsened. He was gasping. A doctor in Bengaluru, guiding them over the phone, advised them to stop at a nearby teaching medical college hospital. He was stabilized there for a few hours. Then the family continued the journey and finally reached a corporate tertiary care hospital in Bengaluru.
That journey took more than forty hours…!
Forty hours is not a number when a nerve disease is moving toward the lungs. Forty hours is not distance on a highway. It is biology (pathology) unfolding without permission. It is oxygen, panic, traffic, waiting, pleading, calling, guessing, hoping. It is a family sitting beside a deteriorating teacher, trying to understand whether they are moving toward safety or merely moving.
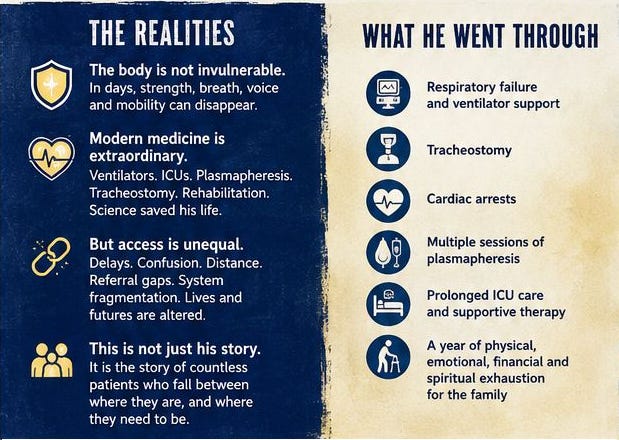
In the months (to be precise 13 months) that followed, he went through tracheostomy, cardiac arrests, prolonged intensive care, multiple sessions of plasmapheresis, supportive treatment, nursing care, physiotherapy and a year of uncertainty that no discharge summary can contain. His body fought. Medicine fought. His family fought. There must have been days when one vital sign felt like victory, and days when a small setback must have felt like betrayal.
He survived.
That sentence deserves respect.
He survived because modern medicine exists. He survived because ventilators exist. He survived because intensive care exists. He survived because plasmapheresis exists. He survived because tracheostomy, monitoring, antibiotics, suctioning, nutrition, physiotherapy and rehabilitation exist. He survived because nurses, intensivists, neurologists, physiotherapists, technicians, family members and invisible hands kept him alive when his own body had almost withdrawn cooperation.
It is fashionable now to speak of hospitals, doctors, pharma and modern medicine only through suspicion. Some suspicion is earned. Healthcare has commercial excess, institutional arrogance, poor communication, avoidable delay and ethical blindness. But criticism becomes foolish when it forgets the obvious: a 65-year-old man with severe Guillain-Barré syndrome, respiratory failure, cardiac arrests and prolonged ICU dependence surviving for a year is not a small thing. It is a triumph of science, skill, endurance and human labour…!
Modern medicine did not fail this man. It pulled him back from death.
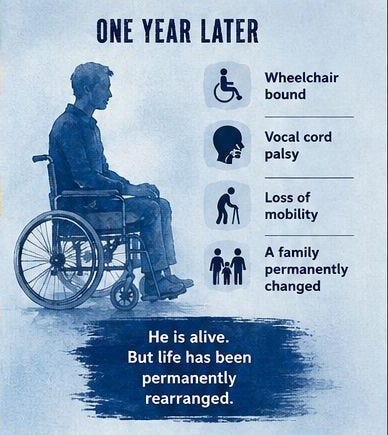
But survival is not the same as return.
Today, after one year, he is wheelchair-bound. He has vocal cord palsy. He has lost mobility. His life has been rearranged by one illness. His family’s life has also been rearranged. In chronic neurological disability, the patient is not the only patient. The family becomes an unpaid ICU, an informal rehabilitation centre, a financial shock absorber, a nursing unit, a transport service, a rehabilitation coordinator, and often, silently, a casualty.
Someone must feed. Someone must lift. Someone must clean. Someone must arrange physiotherapy. Someone must understand prescriptions. Someone must call hospitals. Someone must borrow money. Someone must stop working. Someone must sleep lightly, because the patient may need help at night. Families do not merely “support” such patients. They are absorbed into the illness.
This is what disturbed my colleague. And this is what disturbed me…!
Not because Guillain-Barré syndrome is always preventable. It is not. Not because every patient with GBS can be brought back fully. They cannot. Not because every bad outcome is someone’s fault. That is immature thinking. Disease has its own violence. Biology is not obedient. The human body has limits, and medicine, even at its best, does not erase them.
But some cases do not allow us to hide behind disease alone.
What if the first recognition had been sharper?
What if respiratory weakness had been anticipated earlier?
What if the ambulance had been equipped to support a deteriorating neurological patient, rather than function mainly as a vehicle with a siren?
What if the receiving hospital had been alerted before transfer?
What if the referral had been not just to a bigger place, but to the right place, at the right time, with stabilization and handover?
What if a region with so many hospitals, medical colleges and corporate centres had a referral network humane enough that a frightened family did not have to depend on a stranger’s voice on the phone to find its way?
These questions are uncomfortable because they produce no clean villain.
The problem is not one doctor, one hospital or one ambulance. The problem is a system in which responsibility becomes blurry exactly when clarity is needed most. Everyone does a part. Nobody owns the whole journey. The patient moves from one institution to another, but the illness does not wait for paperwork, bed availability, geography, institutional ego or the family’s ability to negotiate.
This is one of the great paradoxes of modern healthcare. We have ventilators, but not always timely ventilation. We have neurologists, but not always reachable ones. We have plasmapheresis, but not always where the patient first needs it. We have hospitals everywhere, but not always a system that connects them intelligently.
The body is fragile. That is the first truth.
Most days we forget this. The body obeys so quietly that we mistake its obedience for simplicity. We walk, speak, eat, sleep, teach, drive, write, swallow and breathe without gratitude. Then one immune-mediated storm attacks the peripheral nerves and the fiction collapses. Suddenly, every ordinary act reveals itself as a sophisticated biological achievement. Breathing is not simple. Swallowing is not simple. Standing is not simple. Voice is not simple. Life is not simple. It only appears simple when the body is kind.
The second truth is that modern medicine is astonishing.
A century ago, many patients with severe neuromuscular respiratory failure would simply have died. Today, a patient can be ventilated, fed, monitored, protected from infection, treated with plasma exchange or immunoglobulin, rehabilitated and kept alive through a storm that would once have been fatal. This is not sentiment. This is science turned into infrastructure. A ventilator is not just a machine. It is physiology made mechanical. An ICU is not just a room. It is organized vigilance.
But the third truth is harsher.
Modern medicine can save a life, while the healthcare system wounds the same life through delay, confusion, poor triage and abandonment disguised as referral…!
This is where the ethical question begins.
Medical ethics is not only consent forms, confidentiality and signatures. Those matter, but they are not enough. In an emergency, ethics lives in recognition, communication, stabilization, transfer and ownership.
Do we recognize severity early?
Do we tell the family the truth without either panic or false reassurance?
Do we stabilize before sending?
Do we call ahead? Do we document clearly?
Do we transfer to the correct level of care? Do we make sure the ambulance can handle what may happen on the road?
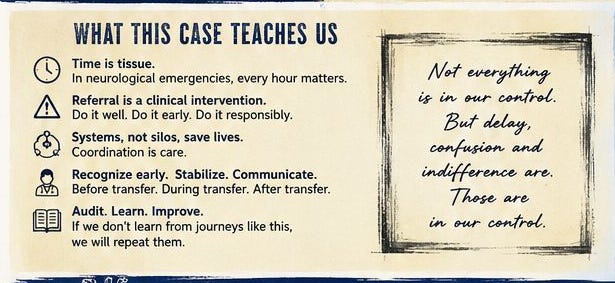
Referral is not clerical work. Referral is a clinical intervention…!
Done well, it saves. Done badly, it becomes risk displacement. A patient is moved, but responsibility is not. A name is written, a destination is suggested, an ambulance leaves, and everyone feels that something has been done. But the patient’s biology continues in real time. In Guillain-Barré syndrome, time does not behave like a calendar. It behaves like nerve conduction, respiratory muscle strength, swallowing safety and autonomic instability. A few hours may mean little in one patient and everything in another.
This case also exposes a middle-class (in particular) illusion about healthcare: that Grand looking hospitals mean healthcare exists….
They do not.
A city may have medical colleges, private hospitals, specialists, diagnostic centres and ICUs, and a patient may still be functionally alone inside that abundance. Healthcare is not the presence of buildings. It is the reliable movement of the right patient to the right care at the right time, without forcing the family to become logisticians during a medical emergency.
We see versions of this all the time. A child with sepsis. A pregnant woman with eclampsia. A stroke patient. A newborn with respiratory distress. A teacher with ascending paralysis. The story changes, but the pattern is familiar. The disease begins. The family searches. The first facility hesitates or refers. The ambulance is uncertain. The receiving centre is not ready. The definitive care comes late. Science rescues what it can. The family pays for what the system did not organize. Later, everyone calls it fate.
Some of it may be fate.
But not all of it.
That distinction matters. If we call everything negligence, we become unfair and stupid. If we call everything fate, we become morally useless. The truth is harder. Some damage comes from disease. Some comes from delay. Some comes from the randomness of access. Some comes from the fact that healthcare is still designed around institutions rather than around the patient’s journey through them.
The patient does not experience healthcare as departments, buildings and referral letters. The patient experiences it as a chain. One weak link can change a life.
What should disturb us is not only that such stories happen. What should disturb us is that we have grown used to them. We discuss them in corridors, shake our heads, praise the final centre, pity the family and move on. We have blame culture when something becomes public, and silence culture when it does not. What we do not have enough of is just culture: the discipline to examine a bad journey honestly, without immediately hunting for a scapegoat or protecting reputation.
A serious healthcare system would study such journeys.
Where was severity first recognized?
Was respiratory function assessed?
Was the transfer appropriate?
Was the ambulance equipped?
Was the receiving unit informed?
Was the family counselled?
Could the patient have reached definitive care earlier?
Not to punish blindly. Not to shame individuals. But to stop pretending that a patient’s path through the system is someone else’s problem.
This one case contains everything: the fragility of the human body, the power of modern medicine, the exhaustion of families, the ethics of referral, and the unfinished accountability of our healthcare system.
The professor survived. His family survived in another way. My colleague was shaken because he knew the patient not as a bed number, but as a teacher from his own past, a human being whose life had been permanently altered. I was shaken because the story felt painfully familiar. Every doctor has seen versions of it. Every family fears becoming the next version.
There are cases that teach diagnosis. There are cases that teach humility. There are cases that expose the system.
This was all three.
Kudos to the patient and his family for enduring what no family should have to endure. Kudos to modern medicine for pulling him back from death. Kudos to every nurse, doctor, technician, physiotherapist and caregiver who helped keep him alive through that long year.
But shame on us if we stop at admiration…!
The correct response to such a story is not sympathy alone. It is referral discipline. It is early recognition. It is equipped transfer. It is accountable handover. It is regional coordination. It is the refusal to let another family travel forty hours through uncertainty while a treatable neurological emergency climbs silently toward the lungs.
A human body can fail without warning.
A healthcare system should not…!

Vikram, the part that stays with me is that the disease moved through physiology while the system moved through geography. That mismatch is the whole case. Guillain-Barré was climbing from strength to swallowing to respiratory reserve, on nerve-conduction time. The pathway could only answer in destinations: a referral, an ambulance, a bed. The two clocks were never synchronized.
That is why a transfer can feel like progress. The patient is physically moving, so it seems something is being done. But the forty hours moved his body toward care without moving responsibility along with it. What you are pointing at is a live thread of ownership that stays attached to the patient while the body changes in real time. Referral fails not when the address is wrong, but when responsibility stays behind.